





Introduction
Fractures of the femoral shaft occur more commonly in young patients involved in high-energy traumas, such as motor vehicle accidents or falls from a significant height. These injuries are often observed in polytraumatized patients and may require stabilization in emergency.
Antegrade or retrograde intramedullary nailing (IMN) is the gold standard for the treatment of femoral shaft fractures, with high rates of successful outcomes reported in literature. However, the risk of nonunion or delayed union is not negligible, ranging from 1 to more than 10% according to different authors.1–3
Open reduction and internal fixation (ORIF) with plate and screws is an alternative to IMN in femoral fractures involving the metaepiphyseal region, especially at the distal end. In these injuries, anatomical reduction of the articular fragments is mandatory to recover normal knee function. This procedure is more invasive than IMN, requiring exposure of the fracture site with hematoma drainage and soft tissue dissection.
Several factors can hinder bone healing, such as injury severity, inadequate fracture reduction, insecure fixation, bone loss, infection or devascularization in case of fracture site exposure. In addition, systemic factors (general health, nutritional status, tobacco use) can play a role.
Femoral shaft nonunions are disabling for the patients, with relevant socioeconomic and psychological impairment. Treatment can be challenging and relies on different techniques, either conservative or surgical.4 Among the latter, nail dynamization or nail exchange are relatively simple, but not always feasible or sufficient. In case of previous ORIF, nonunion surgery might require alternative methods of osteosynthesis, with some kind of biologic augmentation if necessary.
The Reamer-Irrigator-Aspirator (RIA) System® (DePuy Synthes, Leeds, England) was initially conceived to provide safer reaming of the medullary canal during IMN.5 The RIA System produces a constant flow of saline solution into the bone shaft, resulting in less thermal damage, and it provides negative pressure to minimize the risk of fat embolism.6 Since RIA allows to harvest large amounts of autologous morselized bone with high osteogenic and osteoinductive properties, its use was gradually expanded to treat bone defects caused by traumas, tumors or infections.7
In this paper, we report the use of the RIA System for the treatment of two complex cases of femoral shaft nonunion, resulting from failed internal fixation with hardware breakage. A review of the published literature on the treatment of femoral nonunions with RIA was also performed.
Case presentation
Case 1
A 35-year-old man suffered a minimal extradural hematoma (< 10 ml) in the right frontal area and a comminuted supracondylar fracture of the right femur following a motor vehicle accident (Figure 1a). Transtibial traction was applied in emergency for temporary fracture stabilization, while the patient was monitored for the neurologic and hemodynamic conditions.

Four days after trauma, the patient underwent osteosynthesis with a 4.5 mm LCP plate® (DePuy Synthes, Leeds, England) and 4 lag screws; synthetic bone chips were used to fill a postero-medial bone defect in the metadiaphyseal region (Figure 1b).
The patient was discharged after 8 days. Knee range of motion (ROM) was gradually increased and partial weight bearing with crutches was started after three months. Walking without aids was delayed because the patient complained of quadriceps weakness caused by femoral nerve dysfunction, which recovered uneventfully 6 months after trauma.
At 9-month follow up, local tenderness was found at the fracture site, knee ROM was 0°-90° with moderate varus instability. CT scan of the distal femur did not show any evidence of bone healing.
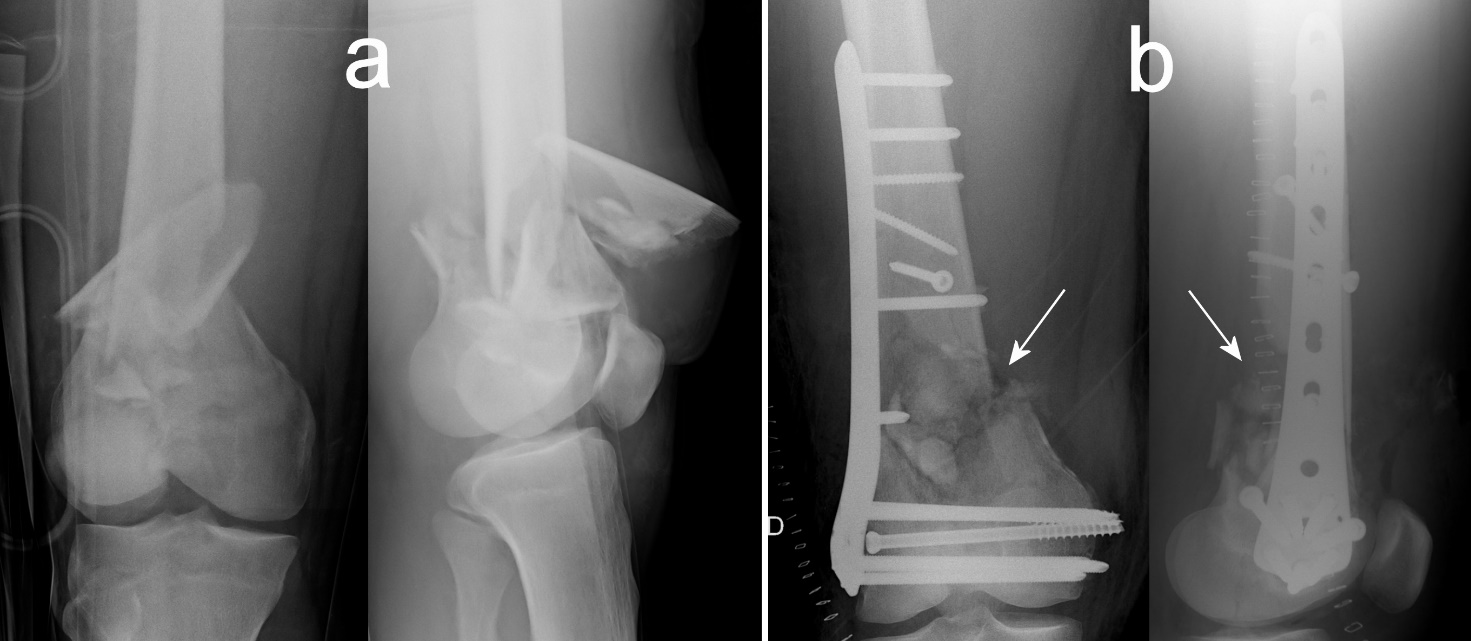
One year after surgery, a revision procedure was performed to treat the femoral nonunion. The plate was not loose and was left in place, since the bone fragments were well aligned and stable. The nonunion site was freshened and filled with autologous tricortical bone graft harvested from the ipsilateral iliac crest and morselized cancellous allograft from two femoral heads (Figure 2a).

Postoperatively, weight bearing was prohibited for 3 months and the knee was gradually mobilized starting from 0° to 45°. During the following months, clinical findings were encouraging: pain subsided, knee function and muscle strength gradually improved. Radiograms showed remodeling and apparent integration of the bone graft.
One year after revision surgery, the patient presented with acute thigh pain and inability to bear weight. X-rays showed distal femoral nonunion with plate rupture (Figure 2b).
Clinically, there were no signs of infection, white blood cells (WBC), C-reactive Protein (CRP), erythrocyte sedimentation rate (ESR) were normal.
Another procedure was then performed: the screws and the broken plate were removed, the nonunion site was freshened and tissue samples were collected; the bone defect was filled with 55 ml of autologous morselized bone graft harvested with RIA System from the contralateral femur. Fixation was achieved with a NCB distal femoral plate® (Zimmer Biomet, Warsaw, IN – U.S.A.) with 5 diaphyseal and 6 epiphyseal angle-stable screws (Figure 3a).

The intraoperative findings were not indicative of infection and the culture of the tissue samples collected at the time of surgery were negative for bacteria presence.
Knee mobilization in a brace and toe-touch weight bearing with two crutches were allowed one week after surgery and full weight bearing at 3 months. No weight-bearing restrictions were prescribed for the left femur at any time.
Radiographically, bone union was evident 10 months after the RIA procedure (Figure 3b). At two-year follow up (four years from trauma), the patient was in good health but complained of moderate right knee pain and slight limping with full weight bearing. He also reported recurrent pain at the iliac crest harvest site with paresthetic meralgia, while no symptoms appeared on the left side after RIA. There was a shortening of the operated limb of 1.5 cm. Hip and knee flexion were both limited to 90° (Figure 4). The scores of the rating scales used to assess the clinical status were the following: 72/100 for the Harris hip score (HHS),8 51/100 and 80/100 (Knee score and Function score, respectively) for the Knee Society Score,9 and 59/100 for the WOMAC knee index.10
.jpeg)
Case 2
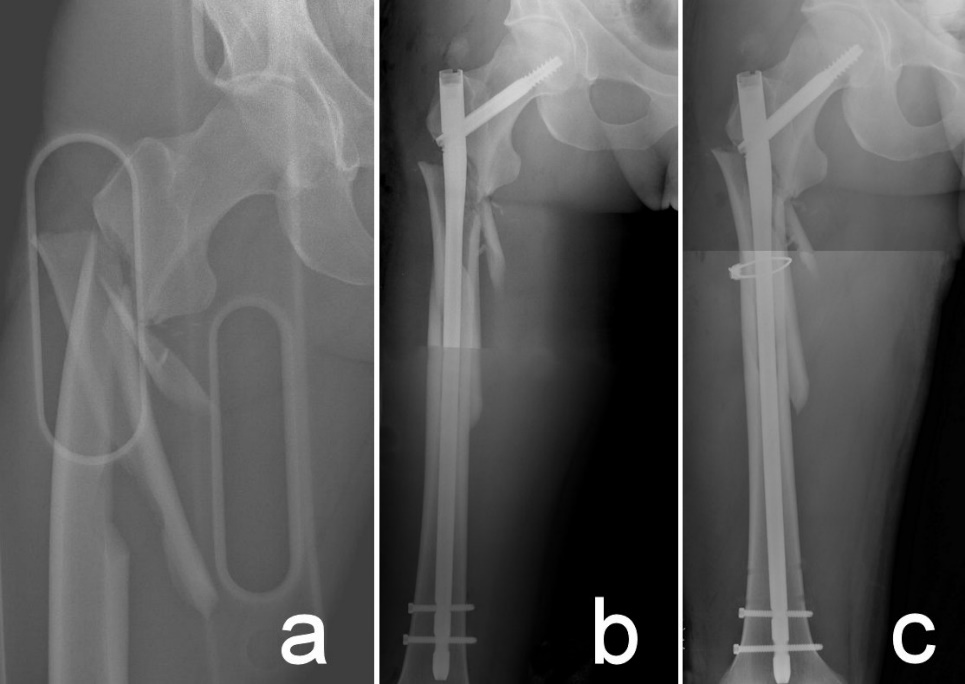
A 27-year-old man sustained a motor vehicle accident and was diagnosed with a multifragmentary subtrochanteric fracture of the right femur (Figure 5a) and avulsion of the anterior superior iliac spine on his left side.

After hemodynamic stabilization and support with blood transfusions, the femoral fracture was fixed with a long cephalomedullary nail (Gamma nail®, Stryker, Kalamazoo, MI – U.S.A.) (Figure 5b). Since the reduction achieved was unsatisfactory, with 2 cm lengthening of the femur, it was decided to perform revision surgery after 9 days. A free diaphyseal fragment was reduced and fixed with a wire cerclage, and the femoral length was restored without removing the nail, but just sinking it down into the distal fragment by pushing the femur from the knee after distal screws removal (Figure 5c).
After discharge from the hospital, the patient did well and underwent periodical clinical and radiographic controls. Partial weight bearing on the operated limb was allowed three weeks after surgery and full weight bearing at three months.
After 7 months, the patient complained of sudden thigh pain while walking. Radiographs showed nonunion of the proximal femur with concomitant nail breakage (Figure 6a).

The presence of infection was excluded with blood tests: PCR, ESR, WBC and procalcitonin were negative. Clinically, the patient was apyretic and without signs of local complications.
Surgery was scheduled two days later and the procedure was performed through a lateral approach to the femur. The broken nail was removed using a previously described technique.11 After exposure of the nonunion site, the interposed fibrous tissue was removed, the medullary canal was reamed and the bone fragment extremities were decorticated, no signs of infection were found intraoperatively. The nonunion gap was filled with 50 ml of autologous morselized bone graft harvested with the RIA System from the left femur. Fixation was achieved by means of a 4.5 mm LCP proximal femur plate® (DePuy Synthes, Leeds, England) (Figure 6b).
In the postoperative period, the patient was transfused with a total of 4 units of concentrated red blood cells and 800 ml of plasma, since the hemoglobin level dropped to 6.4 g/dl. The surgical wound healed uneventfully. Partial weight bearing on the right lower limb was allowed one month after surgery and full weight bearing without aids at 3 months. No weight-bearing restrictions were prescribed for the left femur at any time.
Radiograms taken one year postoperatively showed bone healing of the nonunion (Figure 7). At two-year follow up (31 months from trauma), the patient complained only of slight pain in the trochanteric area and showed excellent functional recovery of the inferior limb (Figure 8), with the following clinical scores: 96/100 for the HHS and 94/100 for the WOMAC hip index.12

.jpeg)
Discussion
The incidence of femoral shaft nonunion after IMN ranges between 1% and 10%, but can exceed 20% in case of subtrochanteric fractures.13 High-energy injuries and open fractures are associated with higher rates of femoral nonunion.14,15 The condition is very disabling and might have a severe impact on health-related quality of life. Treatment options are influenced by pathomechanical, anatomical, and clinical factors.
In hypertrophic nonunions, bone ends are vascularized and capable of biologic reaction, but cannot accomplish bone bridging despite the formation of abundant callus.16 Treatment of hypertrophic nonunions usually requires a more stable fixation: nail exchange is the most common option after IMN, but some authors advocate augmentation plating as a valid alternative.17,18
Atrophic nonunions are typically caused by biological impairment of the fracture site, but also mechanical factors can play a role. Soft tissue trauma, extensive periosteal damage, fracture comminution and exposure are risk factors for the devitalization of bone fragments.19 Bone ends are inert and there is no evidence of callus formation; sometimes a large gap between bone fragments is present. For the treatment of atrophic nonunions, stabilization alone is not sufficient, but biological enhancement is necessary to achieve bone union.16
Autologous bone graft is the best substrate to enhance bone healing, because it gathers osteogenic, osteoinductive and osteoconductive properties.20,21 The iliac crest is currently the most common source for obtaining autogenous grafts since bi- or tricortical grafts can be used to improve the immediate strength of constructs (“bioplating”). Anyway, several studies suggest that cancellous bone is eight times as metabolically active as cortical bone and has greater cellular diversity and activity.22 Moreover, iliac crest bone graft (ICBG) harvesting carries a risk of different complications, such as donor site pain, gait disturbance, pelvic instability, heterotopic bone formation, thigh dysesthesia and ilium fracture23–26 and in several conditions, it may not provide a sufficient amount of bone.21,27
The RIA system is an alternative to ICBG when large volumes of autologous bone graft are required to fill skeletal defects secondary to different conditions or to enhance bone healing in nonunions or joint fusions. In our experience, the RIA system allowed to treat successfully two complex femoral nonunions, both resulting from failed fixation and characterized by hardware breakage. No complications were observed in the postoperative period and no weight-bearing restrictions were prescribed after RIA.
A meticulous surgical technique is necessary to avoid potential complications. Several tips and recommendations aimed to reduce morbidity after RIA have been emphasized in previous papers.28–31 It has been reported that RIA causes less residual pain and requires a shorter harvest time compared to ICBG,32,33 at the cost of a higher risk of blood loss and need for transfusions.34
The expected reduction in donor site morbidity is consistent with our own experience: one of our patients complained of iliac crest pain and paresthetic meralgia after failed ICBG, while he was completely asymptomatic on the side where RIA was performed.
In order to compare our results with other published data, we performed a literature search using the following Mesh search terms, both separately and combined: “RIA System”, “Reamer-Irrigator-Aspirator”, “intramedullary bone graft”, “aseptic nonunion”, “fracture nonunion”, “pseudoarthrosis”, “femur” and “femoral shaft”. The search was limited to adult humans in the PubMed/MEDLINE and EMBASE databases. Studies were searched in the period from January 2000 to April 2020. The obtained reference list of retrieved publications was manually checked for additional references potentially meeting the inclusion criteria and not found by the electronic search.
We included all in vivo clinical studies that assessed the results of treatment of aseptic femoral nonunions (from the subtrochanteric to the supracondylar region) with the RIA System. All papers written in English and published in extenso were considered eligible for the review, with exception of case reports. Septic nonunions, pathological fractures, nonunions of other bone segments and studies performed on animals were excluded.
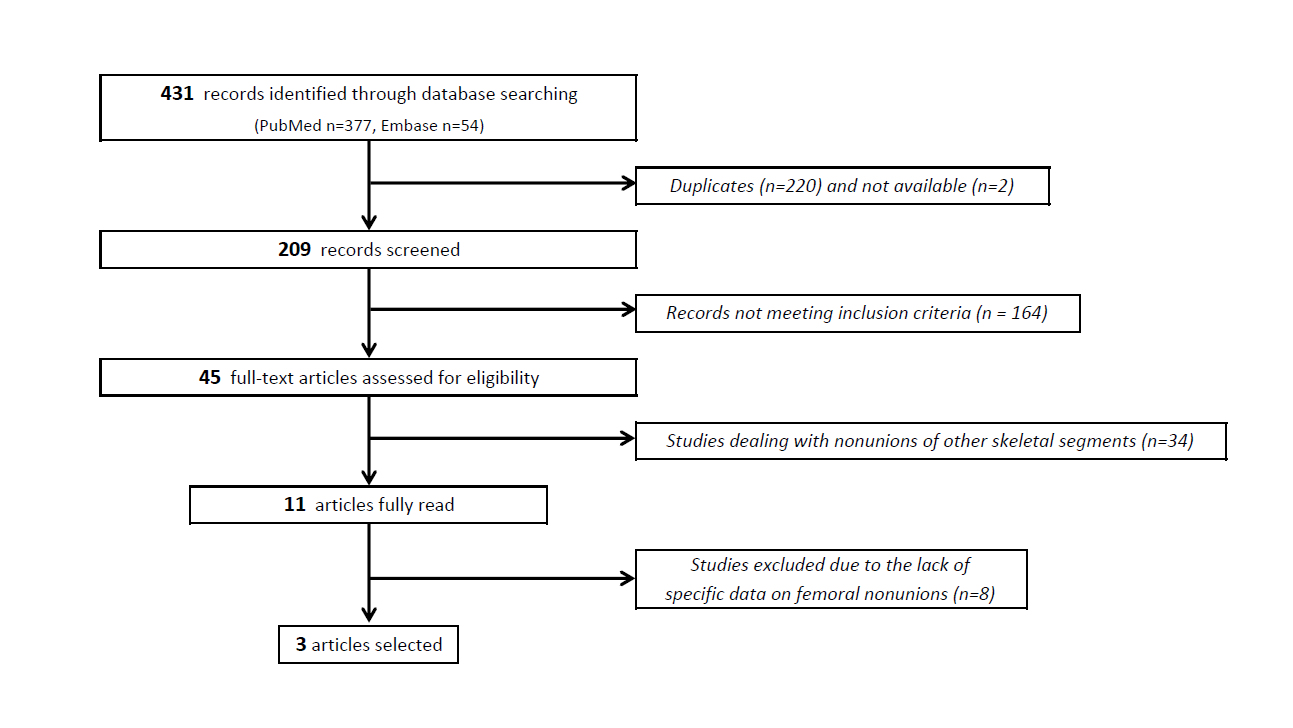
Our literature search identified 431 possible eligible articles, but only three retrospective studies eventually fulfilled the inclusion criteria and were considered for analysis (Figure 9).

Holzman et al. reported on a series of 23 nonunions of the distal femur, that were treated with a double plating technique either in a one-stage or in a two-stage procedure.35 The RIA System was used in 5 aseptic nonunions and combined to bone morphogenetic protein-2 (BMP-2) in two cases. The average age of the patients was 57 years (range, 37 to 79). Bone healing within 12 months was observed in 4 cases; one patient was lost to follow up. No RIA related complications were observed.
Also the study by Attum et al. was dedicated to the treatment of distal femoral nonunions, but these authors used a combined nail/plate construct as fixation method in association to autologous bone grafting.36 This clinical series included 10 patients with an average age of 56 years (range, 26 to 88). The RIA System was used in all patients and was associated to adjunctive augmentation (allograft, BMP sponge, synthetic bone) in 60% of the cases. Bone union was achieved uneventfully in all patients and there were no complications related to the use of RIA. Relevant differences in RIA volumes (min. 20 ml, max. 80 ml) between patients were reported.
Stafford and Norris reported on a two-stage procedure for the treatment of segmental bone defect nonunions of the femur and tibia.37 The first stage consisted of local debridement and application of an antibiotic cement spacer (Masquelet’s technique); RIA was performed during the second procedure to fill the bone defect after spacer removal. Among a total of 25 cases, only 6 aseptic nonunions of the femur were considered for this review. The mean age of the patients was 32 (range, 20 to 48). RIA was combined to ICBG in three patients. The volume of bone harvested with RIA averaged 47 ml, but the range was not reported. Bone union was achieved in all cases and no complications occurred with the use of RIA.
Overall, a total of 21 patients (mean age 51.3 years) included in this review were treated with RIA for aseptic femoral nonunions. Bone union was achieved in 20 patients (one patient was lost to follow up) and no complications occurred during or after graft harvesting with the RIA System. Other forms of biologic augmentation were used in association with RIA in 11 cases (52.4%).
Other authors reported high rates of successful results in the treatment of bone defects with the RIA system.38–42 However, it was not possible to individuate and extract from these studies the specific information related to the treatment of aseptic femoral nonunions, since the clinical data of patients treated for heterogeneous conditions in various anatomical sites were gathered together.
The RIA System allows to harvest relevant volumes of autologous bone graft, but the amount is variable from case to case according to different factors, like patient’s age or surgical technique. It is advisable to have adjunctive materials, such as allografts or bone substitute, available in the operating room to compensate for the lack of substance due to scarce RIA harvesting.
In conclusion, aseptic femoral nonunions are disabling conditions, which might require prolonged therapies and high costs in terms of human suffering and socioeconomic impact. In case of atrophic nonunions, the RIA System can be used to obtain biologically active tissue to enhance bone healing. The efficacy of RIA is well-known and orthopaedic surgeons should be aware of this powerful tool. Controlled trials should be carried out in the future to optimize RIA application for femoral nonunions and provide more evidence of its efficacy.
Author contributions
Landrino M and Grassi FA conceived the study; Clemente A collected the clinical data; Landrino M, Alberio RL and Grassi FA interpreted the obtained data; Landrino M and Alberio RL wrote the article; Grassi FA supervised the entire process. All authors revised and approved the final version of the manuscript.
Informed consent statement
Consent was obtained from the patients for each surgical procedure, while a different and specific consent was obtained to collect and to publish clinical data.
Conflict-of-interest statement
The authors declare no conflict of interest.
Institutional review board statement
The protocol number of institutional ethics committee approval is 802/CE (study n. 164/20 CE).
CARE Checklist (2016) statement
The authors have read the CARE Checklist (2016), and the manuscript was prepared and revised according to the CARE Checklist (2016).