Introduction
In 2060, in the United States, the estimated population will be older than 65 years about 98 million.1 The simultaneous increase in the number of annual implants and the average age of the population has inevitably led to an increase in the percentage of the population having more than one prosthetic implant. In addition, the incidence of periprosthetic fractures and therefore the presence of implant to fix those kinds of fractures will continue to increase as well.2
Interprosthetic or interimplant fractures of the femur were described by Dave et al3 in 1995 whilst the name “interprosthetic” was introduced by Kenny and Quinlan4 in 1998 to describe a femoral shaft fracture between a total hip arthroplasty (THA) and a total knee arthroplasty (TKA).
In scientific literature, the incidence of interprosthetic or interimplant femoral fracture ranges between 1.25% to 8.8%.2
These fractures are particularly difficult to treat because they occur in elderly with several comorbidities. For this reason, the interprosthetic femoral fracture represents a unique challenge for the surgeon and requires a detailed multidisciplinary management strategy, involving both fracture fixation technique and often complex revision ability. The management issues raised by an interprosthetic fracture between ipsilateral hip and knee devices are yet more extensive.2
According to the standard procedures in these injuries with stable components are usually treated by internal fixation without bone grafting. For fixation, it was exclusively used internal fixation with different locking plates with cerclage, cables and/or interfragmentary screws, and stabilization the long locking plate overlapping any stem with a minimum of four to five holes or at least two cortical diameters. In the prosthesis area, a combination of cables, unicortical locking screws, and/or a locking attachment plate was used.2 Other standard procedures to treat these injuries with loose hip stems were treated using monobloc or modular revision stems.5 This type of treatment included removal of the loose stem, including cement extraction in cases of cemented stems, open reduction and fixation of the fractures with cables or wires, and reimplantation during one-stage exchange. Distal femoral replacement was performed for these injuries with loose knee prostheses.2
Other authors used Tumoral Prosthesis for all femoral to treat these injuries where there is bone loosening or both loose prosthesis or higher grade of osteoporosis.2
The aim of the paper is to target the focus on the bone strut grafting to avoid the metal hardware failure and to achieve the bone healing in these injuries.
Materials and Methods
From January 2013 to December 2019, before the COVID-19 pandemic had begun,6,7 at three Level I Trauma Center we enrolled 11 interprosthetic or interimplant femoral shaft fractures around the orthopaedic devices.
Inclusion Criteria were: Interimplants or Interprosthesic, stable hip and knee device, higher grade osteoporosis
Exclusion criteria included: fractures caused by haematological or oncological pathologies, the age of less than 75, prosthesis with loose components recurrent IFF, treatment of nonunion following the initial interimplants or interprothesic fracture.
All fractures were classified according the Pires et al Classification.8 All anaesthesiologic risk of patients were classified according the American Society of Anaesthesiologists (ASA) classification9
At the admission to the department, we asked all patients to provide us with axial bone densitometry data (DEXA).10 To understand and study the capacity of bone healing in patients, we used the Non-Union Scoring System (NUSS).11
All patients were informed clearly and comprehensively of the treatment and other possible surgical and conservative alternatives. Patients were treated according to the ethical standards of the Helsinki Declaration and were invited to read, understand and sign the informed consent form.
The chosen criteria to evaluate the cases during the clinical and radiological follow-up were: the survival and complication rates after surgery; the objective quality of life measured by Activities of Daily Living Score (ADL)12; The bone healing was measured by RADIOGRAPHIC UNION SCORE (RUS)13 and the bone fracture alignment by X-rays; and postoperative complications. The clinical and radiographical follow up endpoints after the surgery were: 1 months; 3 months; 6 months; 12 months and after the 12 months one check every year. Monthly telephone interview has done after the surgery to monitor the survival.
Ethical Considerations
All procedures performed in the current study were in accordance with the 1964 Helsinki declaration and its later amendments. As this retrospective analysis consists of anonymized clinical routine data. Informed consent was obtained from all individual participants included in the study. Orthopedic unit council provided authorization for this study.
Surgical Technique
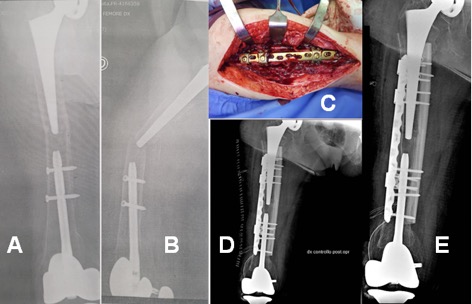
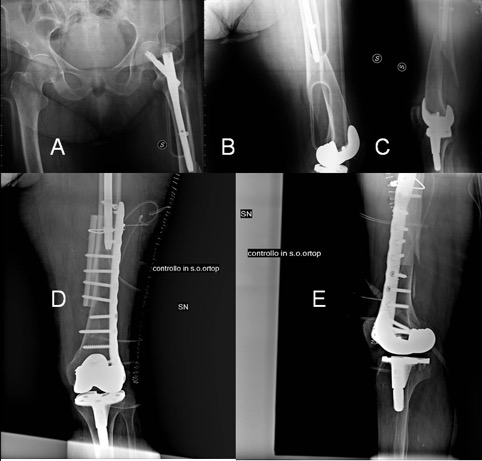
In all cases, the surgeon performed the surgery in a supine position using the direct modified lateral approach to the femoral shaft. All patients underwent to spinal anaesthesia, the antibiotic protocol was 2 gr of Cefamezin 30 minutes before the surgery, 1 gr 3 hours after the surgery and after 6 hours 1 gr of Cefamezin each 6 hours for a day. After exposing the fracture site, it was prepared and the allogeneic bone splint was prepared on a separate table after performing swabs (swab dye tests) for the risk of infection. The modelling of the cortical strut always measured two and a half times the extent of the fracture site and applied on the medial side. The margins of the fracture site were modelled in such a way to create a wide surface for a compression osteosynthesis. The hardware for the osteosynthesis used in all cases was an anatomically pre-contoured low-profile plates LCP® (Synthes™, Oberdorf, Switzerland). At least two compression cortical screws distal and two proximal were also applied to stabilize the strut bone, placed to reinforce the medial wall of the diaphysis and proximal and distal metaphysis. Furthermore, the free space between the strut and bone was filled with allograft morselized bone and bone paste. Finally, the subcutaneous and cutaneous soft tissues were sutured (Fig.1 and Fig.2).
.jpeg)
.jpeg)
Statistical analysis
Descriptive statistics were used to summarize the characteristics of the study group, including means and standard deviations of all continuous variables. The t-test was used to compare continuous outcomes. The exact test was used to compare Categorical variables. The statistical significance was defined as p<0.05. The Pearson correlation coefficient (r) was used to compare the predictive score of outcomes and quality of life. Mean ages (and their standard deviations) of the patients were rounded at the closest year. The predictive score of outcomes and quality of life and their standard deviations were approximated at the first decimal while at the second decimal was approximated Pearson correlation coefficient (r). The reliability and validity of the correlation between osteosynthesis and bone healing were determined by Cohen’s kappa(k). Statistical analyses were performed with SPSS v.15.0 (SPSS Inc., an IBM Company, Chicago, IL, USA).
Results
The average Cortical thickness of femoral shaft was 4.03 (± 1.21; 2.87-6.03) millimeters.
The average point of the NUSS was 58.92(±16.92; range 45-70). The average survival months of the population after surgery was 10.09 (±4.01; range 3-17) (Table 1).
The x-ray reduction after the surgery were: anatomic in 5 cases as good in 5 cases and sufficient in 1 case (Table 1).
After surgery, the average follow up was 9.73 (±3.98; range 3-16) in months while the average death was 10.73 (±3.98; range 3-16) (Table 1).
The average activity daily life (ADL) of the population before the surgery was 2.91(±0.07; range 2-4) while average ADL the population after the surgery was 1.45(±1.44; range 0-3), p<0-05 for the ADL before surgery. The X-Rays Reduction after the surgery was anatomic in 6 cases(p<0.05), 4 good and only 1 sufficient (Table 1). The PS’s X-rays Bone healing measured by RUS occurred in cases on average of 96.3 (±24.2; range 62 -142) days after surgery. The Average Correlation between Osteosynthesis and Bone Healing at the moment of X-Rays Callus were correlated with osteosynthesis were k=0.84 (±0.12; range 0.73-1).
Discussion
In 2014 there was a great interest in the paper by Solarino et al.2 wrote about the controversial treatment for the interprosthetic femoral fracture in this era. Nowadays the orthopaedic surgeons have a new challenge to treat the interimplant fractures.14 The incidence of elective arthroplasty and those treated with fracture implants after lower extremity fractures will continue to increase as well.14 Although fixation strategies exist for periprosthetic hip and knee fractures, there is no standard of care regarding the more complex interprosthetic and interimplant fractures.14 The variety of methods and implants used, and their combinations implies that no “gold standard” exists. The topic is now raising with great interest in the scientific community and clinical practice with fervid literature focusing on the topic. In Solarino et al2 the review it is highlighted that the average patient who suffers from these injuries is fragile very old and suffering from diseases of the bone metabolism, most of the time lured or walking very little and suffering from numerous comorbidities. If we analyse the problems to obtain a correct osteosynthesis of these fractures we find it necessary to implant plaques and screws in malacic bone with a poor seal, femoral canals occupied by stems, nails or cement or types of fractures peri adjacent to both implants (Fig.1). The use of metal cable cerclage should be limited to only one level as their higher rate of ischemia can collapse the medial wall of the femur leading to failure of the osteosynthesis.2,14 Indeed, Peters reported in his 2003 study how important it is to guarantee greater resistance to the medial femoral wall.15 According to our modern experience, lateral plate and medial strut allograft is the best choice to treat the perimplants failure16 and periprosthetic femoral fracture.16–18 The cortical strut only allografts confer stability to the fracture site, and they can incorporate and ultimately increase the femoral bone stock.19 They also “lengthen” the working length of the screws. In scientific literature, only one case in elderly patients has used bone strut allograft for the treatment of inter-prosthetic fracture.20 In our cases series of 11 patients with limited Activities of Daily Living (Table.1), we treated all ORIF and medial graft patients because the main complication leading to re-operations and morbidity or mortality is the non-union or delayed union.21 A recent paper reported the importance of bone strut allografting in the treatment of periprosthetic femoral nonunions.22 The grafting with cortical strut only offers better stability of the construct but from the other side an additional tissue dissection (Fig.2). Wide dissection could result in decreased periosteal blood supply to the fracture site and this can be a reason for of non-union, which can lead to new implant failure and high infection rates after surgical treatment. For this reason, it should be judiciously utilized.23 There is a dynamic change in allograft biomechanics during the incorporation and re-modelling process (Fig.1). Our studies have suggested that cortical struts predictably unite, remodel, mature and not breakage’s risk.16–19 To obtain the maximum stability of the metal-biological construct the osteosynthesis with screws should always be used (Figure 1 and Figure 2) because the use of metal cerclage cables can lead to implant failures and subsequent revisions.22,24 Other authors suggested Total femur replacements or a megaprosthesis are typically reserved for patients with limited bone stock and loose implants or in the situation of multiple failed fracture fixation or persistent fracture non-union, revision to a megaprosthesis may provide a route to definitive treatment.25–27
Conclusion
According to us, the purpose of this surgery is to limit comorbidities and early mortality not to improve optimal restoration of lower limb function. To conclude the data currently available, however, do not yet allow for definitive conclusions about the appropriate treatment and the best choice for Interprosthetic or Interimplants femoral fractures around stable implants regarding complications and clinical outcomes but ORIF with bone allografting is the preferred treatment option for this type of injury to improve osteosynthesis-related outcomes.
ACKNOWLEDGEMENTS
None
AUTHORS’ CONTRIBUTION
G.P., F.L., M.R., L.M, D.D.M, A.S., E.D.C., and G.R. contributed to the design and implementation of the research, to the analysis of the results and to the writing of the manuscript.
FUNDING
None
CONFLICT OF INTEREST STATEMENT
All authors disclose any financial and personal relationships with other people or organizations that could inappropriately influence (bias) their work. Examples of potential conflicts of interest include employment, consultancies, stock ownership, honoraria, paid expert testimony, patent applications/registrations and grants or other funding.
HUMAN AND ANIMAL RIGHT
For this type of study is not required any statement relating to studies on humans and animals. All patients gave the informed consent prior being included into the study. All procedures involving human participants were in accordance with the 1964 Helsinki declaration and its later amendments.