Introduction
Osteoarthritis (OA) is a highly prevalent musculoskeletal disorder with increasing yearly cases. Compared to 2007, OA showed a significant 31.4% increase worldwide.1 OA is the third-largest contributor to the years lived with disability among the musculoskeletal disorders after back and neck pain, accounting for around 7.1% of this burden.2 10-12% of all osteoarthritis cases are post-traumatic (PTOA).3 OA’s first symptoms can appear ten years after injury in patients with PTOA. Patients with PTOA are generally younger than those with idiopathic OA.4–7
Different knee injuries are considered significant risk factors for PTOA.7–9 A meta-analysis, including 20,997 individuals, concluded that a history of knee trauma, mainly Anterior Cruciate Ligament (ACL) rupture, meniscus rupture, and tibial fractures, can increase the chances of having OA more than five times.10 Similarly, a recent report from a longitudinal cohort in Sweden found that after 19 years of follow up, there was a six-fold increase in the risk of knee OA in subjects that sustained a knee injury compared with those without injury. They and other authors found a higher risk for those with a combined ACL injury and meniscal tears than ACL or meniscal tears alone. Fracture of the upper end of the tibia/patella was the third most crucial mechanism.11,12
Subjects with some occupations, like athletes or military work, are at increased risk of a knee injury and subsequent PTOA. The prevalence of knee osteoarthritis in former athletes was 30% in a meta-analysis including 3100 ex-athletes.13 In addition, knee and hip arthroplasties due to OA are greater among former elite male athletes than among age-matched non-athletes controls.13,14 Evidence suggests that subjects develop OA faster after a knee injury, which is about 4.2 times more likely compared to those without a history of knee trauma.15 Most patients with acute ACL tears are younger than 30 when it occurs. The reported incidence of posttraumatic osteoarthritis (PTOA) following ACL injury is 87%, which is very high compared with 19.2% in all adults older than 45 years.16 However, this number will depend on whether the menisci were excised (87%) or preserved (26%).17 Other less common injuries might cause OA and more severe functional consequences for the affected patients. However, the literature is sparse, and there is less research on PTOA due to other traumas than ACL and meniscal lesions. Most research in patients with PTOA has focused on a few types of knee injuries, and limited epidemiologic data is available regarding post-traumatic hip OA. Musculoskeletal injury is considered a predictor of hip OA, with a fivefold increase in risk compared to those without injury.18 Approximately 2% of all hip OA cases are post-traumatic, but no reliable estimates exist.19 Despite its importance, there is insufficient literature analysing the injuries causing PTOA of the hip and their associated risk factors.
This work aims to review the existing literature on musculoskeletal injuries associated with post-traumatic hip and knee osteoarthritis and their associated risk factors to determine those with a worse prognosis.
Methods
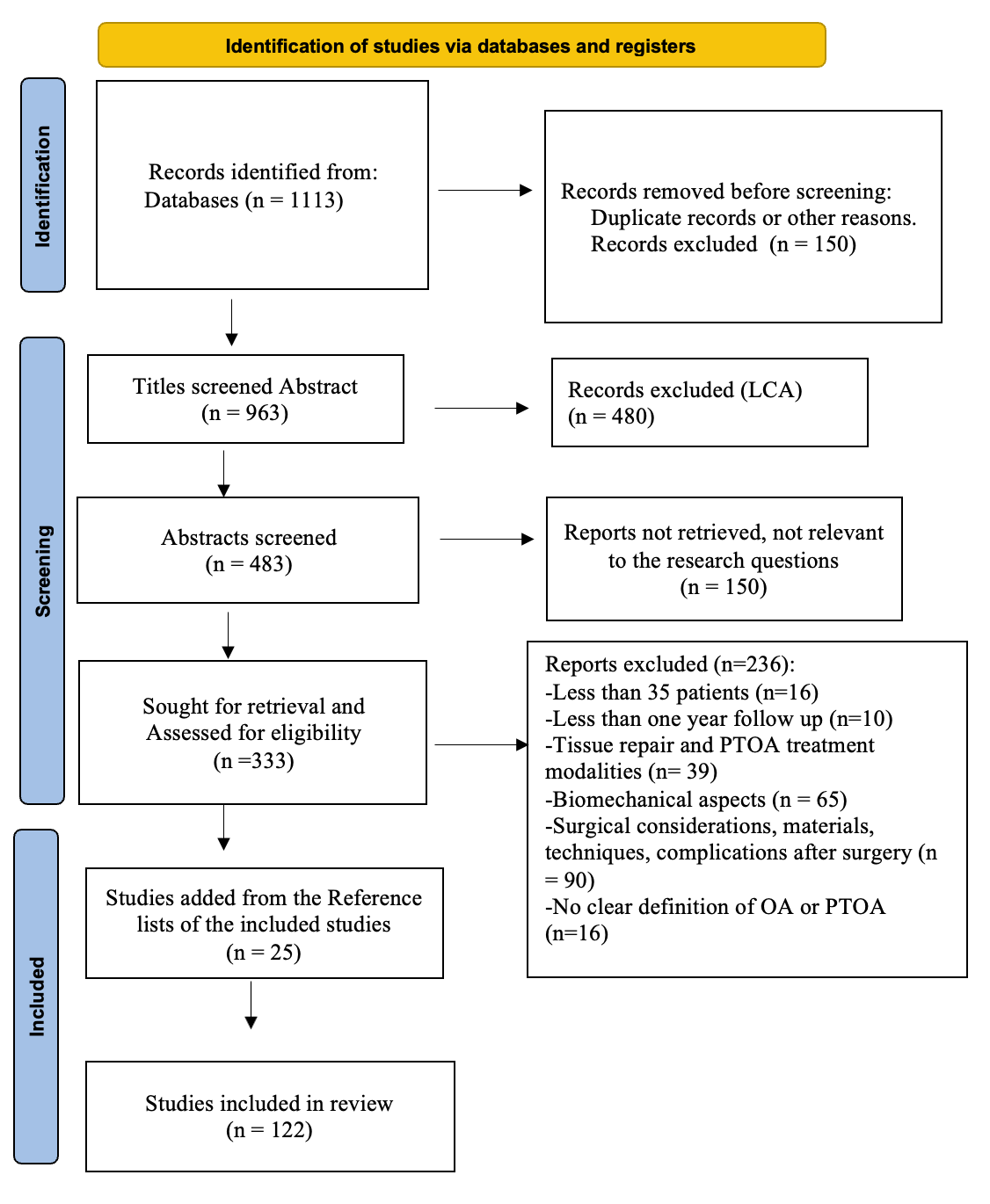
A search of studies published regarding the most relevant injuries and risk factors associated with PTOA was conducted using PubMed, Medline, Embase, Cochrane Library, Google Scholar, and by hand-searching through reviews that were considered a searching method for other relevant articles. This narrative review was performed following a systematic search for articles according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guideline for identifying, screening and including articles. Three reviewers (M.C.B., C.L.M. and C.R.M.) searched using the words: “posttraumatic” (or post-traumatic) AND arthritis OR osteoarthritis, AND hip or knee in the Title/Abstract. We selected human studies published in English in the last 20 years (Till January 2022), with full text available, and only adults. Case reports, letters, clinical trials, and editorials were excluded. Figure 1 presents the literature search strategy and exclusion criteria from the articles retrieved in the initial search. We identified and screened 1113 titles and abstracts for post-traumatic knee (834 articles) and post-traumatic hip OA (279).

After removing duplicate records (n=150) and articles concerning ACL injuries (480 articles), four hundred eighty-three abstracts were screened (n=483). Hundred fifty reports were not relevant to the research questions and were excluded. Three observers analysed the remaining 333 remaining articles. We excluded publications that referred to only osteoarthritis without PTOA cases or other factors that would affect the risk of OA after injury (Figure 1). Our inclusion criteria were: a clear definition of OA, clear identification of posttraumatic osteoarthritis cases and the specific type of injury, including more than 35 patients in clinical studies, and retrospective or prospective studies with a follow up of more than one year. At that stage, 236 articles were excluded. Reference lists of all included studies (n=97) were manually screened for additional articles that met inclusion criteria, adding twenty five more articles. One hundred twenty two articles were included in the review. The three reviewers evaluated each article according to the scientific content, and to classify them were divided into major topics according to the traumatic injuries concerning PTOA. Meniscal tears, proximal tibial fractures and patellar dislocation for knee PTOA. Acetabular fractures, femoral fractures and hip dislocations were the principal injuries for hip PTOA.
Results
Meniscal Tears
Meniscal tears in the presence of ACL injury are as high as 79%, even higher for those with more than eight weeks of trauma.20 Acute injuries occur more frequently in active young patients and chronic degenerative injuries in older patients, where incidental findings of meniscal tears or destruction are common in patients with or without knee pain and OA.21,22 Meniscal tears are more prevalent in men than women, with an annual incidence between 0.3 to 0.7 per 1000 inhabitants.23–26 A medial or lateral meniscal tear is a common finding in asymptomatic subjects but is more common in patients with symptomatic osteoarthritis.21,27 Meniscal damage (grade ≥1) and meniscal extrusion are more frequent in knee-OA cases than in controls (54% versus 18%; and 52% versus 29%).21 The severity of meniscal damage defines the risk of OA. For a minor meniscal tear versus no meniscal damage, the odds ratio (OR) was 3.0 (95% CI: 1.4–6.4); for more severe meniscal damage versus no damage, the adjusted OR was 7.9 (95% CI 4.4–14).21 After 19 years of follow up of meniscal tears, the corresponding risk difference was 10.5% (95% CI 6.4% to 14.7%) compared with uninjured subjects.11
The higher risk for OA is principally seen in patients after meniscectomy, with rates between 24% after four years and 71% after 20 years being higher for total than for partial meniscus repair.22,26,28–31 So far, arthroscopic surgery did not demonstrate to be more effective than conservative management in preventing PTOA.30,32,33 Female sex, obesity, and age 40 or more are risk factors for PTOA after meniscal injury and repair.26,34–36 There are some similarities with the OA risk factors for ACL injuries, perhaps because meniscal tears are commonly associated with ACL ruptures.
Proximal Tibial Fractures
The tibial plateau fractures (TPFs), also called proximal tibial fractures (PTF), represent 1% of all fractures in all age categories, and 8% of all fractures in individuals over 65.37–39 These fractures have an incidence of 0.1-0.13 per 1000 inhabitants and are more common in males than females, principally due to high energy trauma and in women after 70 years secondary to falls.38 For displaced PTFs leading to joint instability, operative treatment is preferred. Open reduction and internal fixation (ORIF) is used to regain normal tibial anatomy, principally for displaced intra-articular tibial plateau fractures.40 Although this procedure might restore normal knee function, PTOA is a common complication following PTFs that may lead to total knee replacement as a secondary treatment (TKR).39,41,42 Tibial plateau ORIF was associated with an approximately fivefold increased risk of TKA in a cohort of 8,426 patients receiving ORIF for tibial plateau fractures.42 A study with 7,701 patients with PTF determined the risk of TKR following proximal tibia fracture (PTF) over five years (SD±3) follow up.43 TKR was performed in 340 (4.3%) patients with a prior PTF after a mean of 2.1 (SD 2.0) years post-fracture, 60% in the operatively treated group versus 40% in the nonoperatively treated group.43 Similarly, in another study with 288 cases of TPF, 4.5% of patients underwent one of the reconstructive procedures for end-stage OA just after two years of the fracture.44 The authors concluded that operative treatment, female sex, and high age were risk factors for TKR after PTF.43 In an older study, female sex and obesity were risk factors for conversion to TKR.45 PTOA is generally estimated to occur in approximately 23% to 36% of cases following intra-articular fracture (IAF).39,41,46–49 However, radiological signs of osteoarthritis have generally been reported in 10% to 83% of studied cases with tibial plateau fractures.37,39,49–52 In a prospective matched case-control study with 48,791 patients with knee fractures, patients with knee fractures had a 3.7 times greater risk of TKR in the first three years after knee fracture, and the risk remained higher throughout their life when compared with the population in the controls group, without fractures.53
In most of those studies, the incidence of OA is predicted by the severity of the lesion, usually determined by Schatzker’s grading system classification for TPFs.47,54–56 It means that those patients with more severe fractures, comminuted fractures (Schatzker types V and VI) or complete articular fractures and fractures with articular depression > 2mm will have the worst prognosis regarding OA.51,54 The included studies showed that this type of trauma has a higher incidence in males and females older than 50.38,54,57–59 In addition, it seems that unicondylar fractures have better functional results after treatment than bicondylar fractures in younger patients.39 Older age might have a worse functional outcome in treated fractures.60,61 The probability of early OA increases with older age at the time of injury, fracture comminution, and comorbidity.42,61,62 As for other knee injuries, a high BMI negatively affects functional outcomes and scores after surgical treatment of TPFs.54,63
On top of the severity of the fracture, including concomitant fractures, knee malalignment, including a deviation of the mechanical axis in varus, step-off and meniscus lesion, might increase the risk of having osteoarthritis at follow up.39,54–56,59,64 Treatment options include open reduction and internal fixation with or without arthroscopy. Closed reduction with percutaneous fixation is considered if the meniscus is intact at arthroscopy.47 Open anatomic reduction with internal fixation is the treatment of choice for articular fractures. However, non-operative management or primary arthroplasty are considered.41,64,65 Outcomes after internal fixation of intra-articular fractures of the distal femur are good, with a low rate of subsequent TKA.45,65–67 However, despite a good to excellent functional outcome in patients younger than forty years, it has been reported that between 23% to 50% of patients might present moderate to severe signs of OA after one year to 14 years of surgery.46,47,68
Regarding surgery, preserving stability and alignment are very important for preventing PTOA of the knee.39,40,62 The association between joint stability and the development of PTOA has been well established.69
Comparing the conversion rate to TKA between tibial plateau fractures and distal femur fractures, the conversion rate for tibial plateau fractures is higher at 4.5% compared to 2.3% for distal femur fractures.70
Patellar Dislocation
Acute patellar dislocation represents 2% to 3% of knee lesions and is the second most common cause of traumatic hemarthrosis of the knee.71 In the long term, acute patellar dislocations can result in patellar instability with recurrence rates of 15% to 44% after non-operative treatment, pain, inability to return to sports as high as 55% of cases, and patellofemoral OA.72 Subjects with patellofemoral instability are more likely to be female, older, and genetically more prone to dislocation.73 Patellar dislocation occurs more frequently in active young individuals practising sports, and females have a 33% higher risk of patellar instability and dislocation than males. Generally, rates for patellar dislocation are between 0.058 and 0.070 per 1000 person-years in the general population.73 This rate has been higher in the aged 10-17 years: 0.29 per 1,000 patient-years, and military personnel: 0.69 per 1000 person-years than in the general population.74,75 Cartilage lesions are common after patellar dislocation and appear to increase with the frequency of dislocation.76,77 The risk of OA increases with the number of years after dislocation as well. Studies with only two or five years of follow up showed no significant increase in OA compared with patients with other patellofemoral problems.73,77 After thirteen years, OA risk is around 22%, and it achieves 50% after 25 years of follow up, depending on whether patients had a recurrent dislocation and the type of treatment received.78 Chronic dislocation, osteochondral injury, trochlear dysplasia, female sex and older age are risk factors for PTOA in these patients.76,78,79
Non-operative treatment is recommended for patients with traumatic, first-time patellar dislocation.71,80 However, in some cases, conservative treatment can lead to recurrent instability. No evidence exists that stabilising patellar surgery by different procedures would decrease the long-term risk of OA.79,81–83 On the contrary, some studies have also shown increased osteoarthritic changes following different operative interventions.81,84 Cartilage lesions were found on magnetic resonance (MR) images from 78% of patients who underwent patellofemoral stabilizing surgery after 12 years.81 In another study, 28% of patients presented full-thickness patellofemoral articular cartilage lesions after a median of seven years follow up. However, the lesions were considered unrelated to the treatment form. The patients were randomly allocated to be treated with initial surgical stabilization or managed with an orthosis without significant differences at the end of the follow up between these groups.81 Finally, it is essential to consider that no trials examined people with recurrent patellar dislocation comparing surgical and non-surgical interventions and long-term outcomes, including OA.83
Acetabular Fractures
The incidence of acetabular fractures is relatively low but has increased in Europe in recent decades. Acetabular fracture represents between 2% to 8% of all fractures, and it has been estimated in around 3-4/100,000 persons/year in the UK and 8.1/100,000 persons/year in Europe.85,86 The most common mechanism for acetabular fractures is high energy trauma and accidents in the young population and low energy trauma such as falling in the elderly. This fracture occurs principally in males and subjects with osteoporosis.85,87,88 Open reduction and internal fixation are suitable for most patients with incongruity or instability of the hip; however, some fractures will require total hip replacement due to OA, principally when residual articular incongruity.89–92 Management of acetabular fractures is complex, especially when it is complicated by central hip dislocation.93 Arthroplasty might be required in between 10% till 30% of cases if the reduction does not reach the required quality.88,89,92–96 Posttraumatic osteoarthritis might occur just six months after the fracture in subjects older than 60. Males are also more affected, as in other cases of PTOA. PTOA might occur after five years of follow up in between 13% to 57% of all cases, including subjects treated with open reduction and internal fixation, principally when the reduction is not satisfactory (>2mm).85,88,89,97–102 Open reduction and internal fixation of displaced acetabular fractures have successfully prevented the need for subsequent total hip arthroplasty (THA) within twenty years in approximately 79% of the patients.95,98,103–105 The quality of fracture reduction seems to be the most important factor that decreases the risk of hip-PTOA.89,99,106 Displacement greater than 2 mm increases the rate of PTOA development after this type of fracture.101,107 The type of fracture influences the quality of the reduction. Both column fractures and type A1 are more common in males, the most difficult, with more significant degenerative changes than other types.103,108
Displacement, intraarticular fractures with fragments, type of fracture (comminuted posterior wall fracture the worst case), and an associated injury (for example, sciatic nerve injury) are associated with a worse long-term functional outcome after acetabular fractures. Further, acetabular fractures with these characteristics present higher complication rates and conversion to late THA90,93,99,109–111. In general, the management options include non-operative measures, open reduction and internal fixation (ORIF), THA, or ORIF with concomitant THA (ORIF-THA). ORIF is considered the standard care for young patients, less effective in older subjects with osteopenia or osteoporosis.112 End-stage OA is the most common complication after ORIF, achieving 36% of the cases, with failure to maintain reduction as one of the contributing factors.113
Male sex, age older than 40 years, obesity, associated chondral or osseous lesions of the femoral head, involvement of the posterior wall and incongruence of the acetabular roof are risk factors for PTOA.89,96,104,105,114,115 Posterior wall fracture is more common than anterior, and patients with this type of fracture have shown higher rates of PTOA when compared with other types of fracture.99,116 In a study with patients older than 60 years, the rate of conversion to THA was 23.6% at 10.5-month postinjury.112 A recent study found that the probability of THA after acetabular fracture increases by 6% per year. It is 21% higher for every mm more in subluxation and approximately 3.5 and 3.7 odds higher when there is the involvement of the posterior wall, contusion and impaction of the femoral head.97 Finally, some authors found no difference in osteoarthritis rates between patients with and without dislocation associated with acetabular fractures.90,109,110,116
Femoral Fractures
Femoral fractures characterized by femoral shaft malunion and malalignment might increase the risk of hip OA and, in less degree, knee OA. Only 8% and 5% of patients with femoral fractures, presented ipsilateral or contralateral radiographic evidence of knee OA after 22 years. However, there were clinical signs and symptoms of OA in 16 patients (26%) who exhibited mild pain or stiffness in the ipsilateral knee.117
Hip fractures are generally less associated with PTOA than acetabular fractures; however, they have a higher incidence. That is the case of the femoral neck and intertrochanteric fractures. Proximal femur fractures are prevalent in the elderly with high morbidity and mortality. They are treated with surgery, usually using intramedullary nails or an extramedullary sliding hip screw.118 Other cases are handled with hemiarthroplasty or total hip arthroplasty (THA), depending on the patient’s condition and the decision of the surgeon.119 In young patients, a hemiarthroplasty is linked to high rates of acetabular erosion and the need for conversion to THA due to secondary osteoarthritis.119 The age-adjusted incidence of femoral neck fractures in the United States is 63.3 per 100,000 person-years for women and 27.7 cases per 100,000 person-years for men.120 Besides, the incidence of trochanteric fractures is about 180–190/100,000 in men and 410–440/100,000 in women. A higher incidence of these fractures has been reported in the military, representing 3.5%-8% of stress fractures in military recruits.121 THA is a treatment used not only for acute femoral neck fractures but also for failed osteosynthesis of femoral neck fractures. THA is recommended in the first intention when an acetabular fracture involves the femoral neck in elderly patients. Around 11% of all performed THA are sequelae or failed internal fixation after proximal femur fracture.122,123 Few studies compare the risk of OA after different types of proximal femur fracture, partly due to the high number of cases that undergo THA.
However, it seems there is a tendency for a higher incidence of OA in patients with trochanteric fractures than in patients with cervical fractures.122 A retrospective study followed 417 patients for around 3.4 years (68% women, median age: 78 years) with a minimally displaced femoral neck fracture treated with internal fixation, and found that 0.5% of cases developed PTOA. A study comparing 349 patients with proximal femoral fractures and 112 patients with hip contusion found that the rate of hip OA between patients with these types of fractures and hip contusion were similar, 16% and 18%, respectively.122 Femoral neck fractures are slightly more common than intertrochanteric fractures, and there is little evidence regarding which one has a higher risk of OA.122,124,125 In a study analysing 102 patients after a minimum 2-year follow up, failed internal fixation for hip fracture (38% intertrochanteric- and 72% femoral neck fractures), 32 cases had THA due to PTOA. 25% had a prior femoral neck fracture, and 20% had an intertrochanteric fracture.124 There is no much literature regarding the risk of OA in patients after these fractures because most of them are treated with THA or by hemiarthroplasty.126 In young and middle-aged patients, internal fixation is the preferred treatment option for both injuries to preserve the native hip joint.
Hip Dislocation
Traumatic hip dislocations might be divided into simple or complex when they present with associated fractures. Acetabular fractures are present in up to 70% of patients with traumatic hip dislocations, which might worsen the prognosis.116,127,128 It is essential to consider that posterior hip dislocations are nine times more common than anterior hip dislocations. In most patients, emergent closed or open reduction is initially performed for this type of trauma within 6 hours of dislocation. Hip dislocations are prevalent in younger males between 14 or 16 years to 40, happening in subjects till 72 years.116,129–131 PTOA is the most common long-term sequelae of a simple hip dislocation.116,127,132 Posttraumatic osteoarthritis might usually appear two years after the initial injury, being more common after ten years, where it might be present in up to 24% of cases.116,130,131,133 Some authors recommend a closed dislocation reduction in less than six hours of the injury, considering this a risk factor for bad outcomes, including OA.131 Others recommend arthroscopic repair or debridement of labral tears to reduce the risk of posttraumatic osteoarthritis; however, most authors agree that delayed reduction increases the risk of OA.116,131,134,135
The principal factor associated with the incidence of PTOA in subjects with traumatic hip dislocation is the severity of the injury. Severe injuries are associated with femoral or acetabular fractures and cartilage or osseous fragments, which may inhibit congruent reduction.116,123,136 In a study including 69 patients with “hip joint associated injuries”, assessed at a mean follow-up of 36.9 months after surgery, 12 patients (17%) developed OA, two of them before the first year after surgery. The principal factor common for these patients was dislocation, a high-energy trauma, principally among males with car and motorcycle accidents.137
There are reports of PTOA after anterior dislocation. Rates from 0.12 for dislocation with or without minor fracture to 0.83 for those associated with a femoral head fracture.136,138 Femoral head fracture is associated mainly with posterior hip dislocation. This type of injury is far less common than isolated dislocations or dislocations combined with acetabular fractures representing only 6 to 15% of all types of dislocations however, they are relevant regarding PTOA.123,127,139 PTOA has been reported in between 16-30% of patients with posterior dislocation, rising to more than 50% when associated with femoral head fractures; although the association is rare, it is an incident of 4 to 17% of cases.116,139–142
Determining the Risk of PTOA
According to this review, the likelihood of having OA after injury will depend principally on the type and severity of the trauma, strongly influencing the disease risk estimates.5,7,47,50,51,136,138 Fractures are the most common traumatic mechanism related to PTOA, and this is a predominant injury in males, one of the reasons for having a higher number of males than females with PTOA.15,39,143 Among the studied injuries, meniscal tears have a higher incidence, principally in young population19,35; They also might appear on routinely MRIs of elderly individuals as chronic degenerative injuries.15,26,35 However, in the long term, radiological signs of OA have been reported in up to 83% of cases after proximal tibial fractures and up to 71% of cases of meniscal damage. Patients with a more extensive or complicated fracture will have a worse prognosis, and the probability of developing OA increases with the patient´s age at the time of the injury.4,51,87,107 Acute patellar dislocation is a the less common knee injury and principally occurs in females. The female population has a higher risk of instability and dislocation than men.71–73 Chronicity, advanced age and heavyweight are the main risk factors for patients with patellar dislocation.75,77 Femoral fractures are the most common in the elderly; however, few studies compare the risk of OA after different types of proximal femur fracture because most of these fractures undergo surgical treatment. They are associated with OA to a lesser degree, principally in malunion or failed internal fixation cases. Hip fractures were the most common past injury reported from patients in studies involving PTOA of the hip, and acetabular fractures the most relevant regarding hip OA. Acetabular fractures have a low prevalence (1% of all fractures). However, posttraumatic osteoarthritis after these fractures occurs in between 40 to 50% of the cases, mostly in males.88,89,98 Hip dislocation is another trauma highly associated with PTOA, reported in between 16-30% of cases being higher risk when associated with a femoral head or acetabular fracture.108,109,116,127,128
For most traumatic injuries, operative treatment becomes a risk factor for future PTOA. Meniscectomy is a known factor in increasing the risk of OA, being more common in male patients than in women.5,23–26,28 Operative treatment of tibial plateau fractures is considered a risk factor for PTOA. Tibial plateau ORIF is associated with an approximately fivefold increased risk of TKR.42 In the case of first-time patellar dislocation, conservative treatment is indicated. No evidence that stabilising patellar surgery through different procedures would decrease the long-term risk of OA. In addition, in the case of hip dislocation, authors recommend early reduction, considering that the time between injury and surgery is an essential factor in OA’s trauma recovery and development.89,116,134,135 Other risk factors concerning the operative treatment increase the risk of OA. The most mentioned are residual articular incongruity, instability, reduction quality and delayed treatment.
The time course in which clinically measurable PTOA develops is highly variable, ranging from as few as two years in articular fractures to decades for less severe joint injuries. The presence of additional patient risk factors, such as advanced age, obesity, joint malalignment or genetic risk factors, leads to a more severe outcome. In addition, it is essential to mention that some patients already had osteoarthritis at the moment of trauma, and the new injury can accelerate the progression of OA. Table 1 summarises the principal findings regarding each type of injury.
Authors’ contributions
Conception and design: MCB. Identification, screening and inclusion of articles: MCB, CLM and CRM. drafting of the article: all authors, Critical revision of the article for important intellectual content: CRM and MCB), final approval of the article (all authors).Obtaining funding: MCB.
Disclosures about potential conflict of interests
The authors have no conflicts of interest to declare.
Funding
This work was supported by grant #2016/21039-0, São Paulo Research Foundation (FAPESP).