INTRODUCTION
Fibrous Dysplasia is an uncommon disorder of the bone caused by mutations of the Gsα protein encoded by gene GNAS, in which bone is replaced by fibro-osseous tissue. The disease may be monostotic or polyostotic (PFD), and in some cases may associated with cafè-au-lait skin pigmentation and hyperfunctioning endocrinopathies, such as in McCune-Albright Syndrome (MAS).1–8
The proximal part of the femur is commonly affected. The mechanical stress causes progressive varus and bowing of the bone, resulting in coxa vara and shepherd’s crook deformity, which represent the most common femoral deformities. In some cases, they are associated with further deformities of the diaphysis or of the distal part of the femur. The tibia is also commonly affected, with valgus and/or procurvatum deformities. To the best of our knowledge, two classifications of femoral deformities have been proposed.9,10 Ippolito et al in 20149 identified six reproducible patterns of femoral deformities, after reviewing the radiographs of 127 affected femurs, while Zhang et al,10 one year later, classified 227 femurs in five types. Some deformities may change their pattern during skeletal growth.11 Both classifications analysed the deformities of the femoral neck or of the proximal femoral shaft and are useful in addressing the best surgical correction. The deformities of the knee caused by axial deviation of the distal femur or of the proximal tibia, as well as the deformities of the tibial shaft, have never been classified, and are usually described as secondary deformities.
Surgical treatment of proximal femoral deformities in PFD is technically demanding and the optimal surgical management is still controversial. However, in the majority of cases, cervico-diaphyseal interlocking intramedullary nails are preferred to other devices in stabilizing the corrective osteotomies, because failures are very likely to occur when using screw or blade plates.12–17 However, some authors deem appropriate the use of screw or blade plates in stabilizing corrective valgus osteotomy of the femoral neck.18,19
Some patients affected by PFD may have a genu valgum caused by axial deviation of the distal femur or proximal tibia that are hard to manage using intramedullary nailing. In some cases, knee deformities are difficult to recognize and can get worse after surgical correction of the proximal femoral shaft.9,10 Genu valgum in PFD, may be surgically corrected with medial distal femoral or medial proximal tibial epiphysiodesis if performed during skeletal growth,20 while a varus osteotomy is needed in adults.
The aim of our study was to report the outcomes obtained in a series of adult patients with PFD or MAS operated on for complex deformities of the femur and/or tibia and stabilized with intramedullary nails. An associated residual genu valgum greater than 15° was present and surgically treated by distal femoral or proximal tibial osteotomy stabilized with a screw plate.
MATERIALS AND METHODS
Five patients with PFD or MAS were identified for this study from a pool of patients surgically treated at our Institution between 1998 to 2016. Mean age at surgery was 23.6 years (range 15-37 years). All these patients were operated on by femoral and/or tibial osteotomy stabilized with intramedullary nail. Some cases with severe coxa vara and shepherd’s crook deformity were corrected in two stages, using peripheral plate first and then the intramedullary nail. The inclusion criteria for this selection was the presence a residual genu valgum greater than 15°. In these cases, additional surgery was perfomed, consisting of a distal femoral opening wedge varus osteotomy in three cases and a proximal tibial closing wedge varus osteotomy in the remaining two cases, stabilized in all cases with a peripheral screw plate. Of the three cases operated on by distal femoral osteotomy, two patients showed worsening of their genu valgum after surgical correction of the shepherd’s crook deformity and internal fixation with intramedullary nail.
These five patients were followed up clinically and radiographically to evaluate the correction of the valgus deformity of the knee. From a clinical point of view, we evaluated pre and postoperative pain, range of motion of the knee, presence of limp, limitation in daily and social activities, and satisfaction with the final result. From a radiographic point of view, we evaluated, on weight bearing radiographic examination, the improvement of the anatomic/mechanical axis of operated lower limb, measuring the femoro-tibial angle centred on the knee. Healing of the osteotomy and possible failure of the fixation implant were also investigated.
ETHICAL CONSIDERATIONS
The study has been approved by the ethical committee of our Hospital – Policlinico di Tor Vergata, Rome, Italy. Informal consent was obtained from all partecipants.
RESULTS
The mean age at follow-up was 32 years, while the mean length of follow-up was 8.4 years.
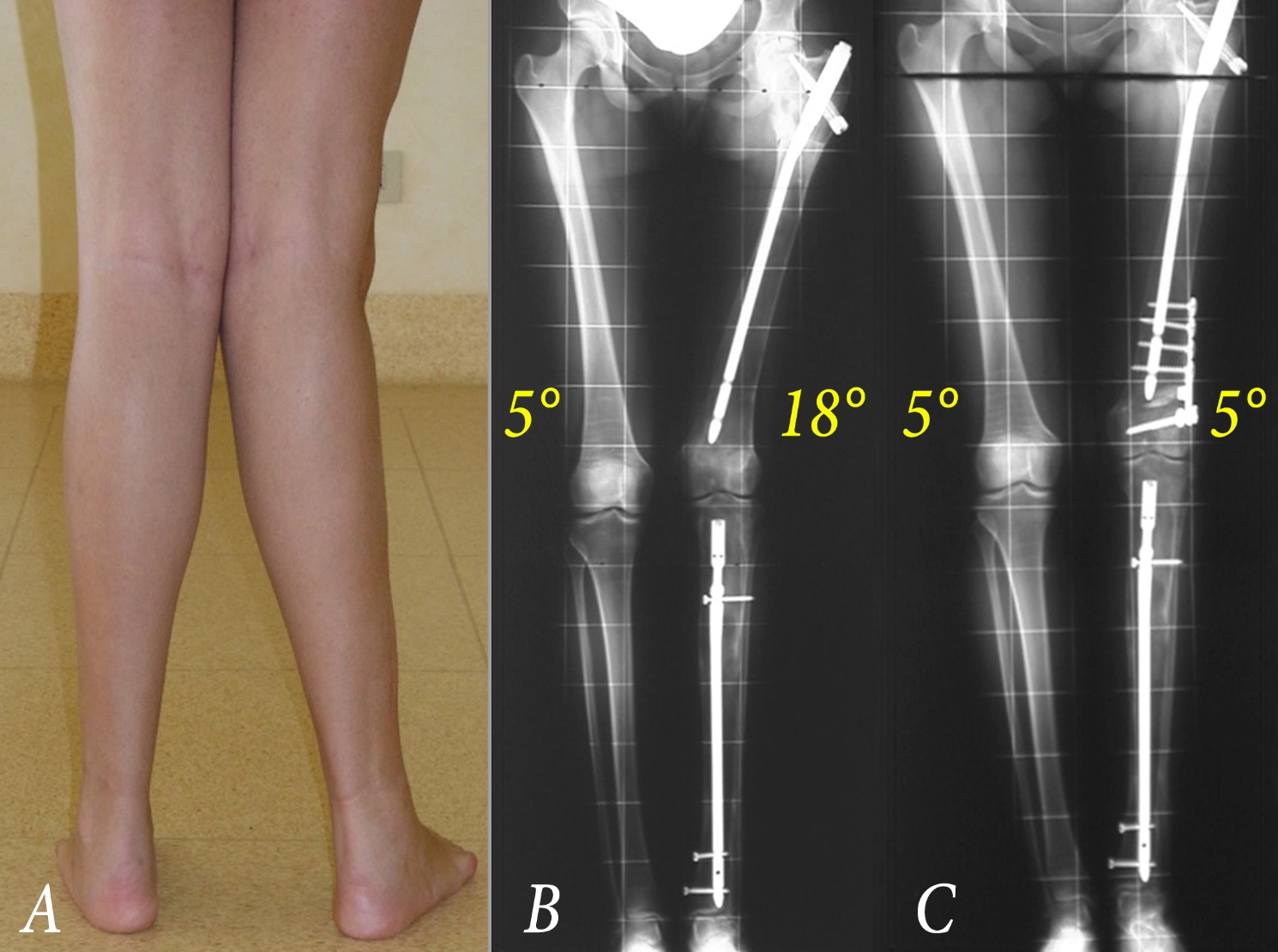
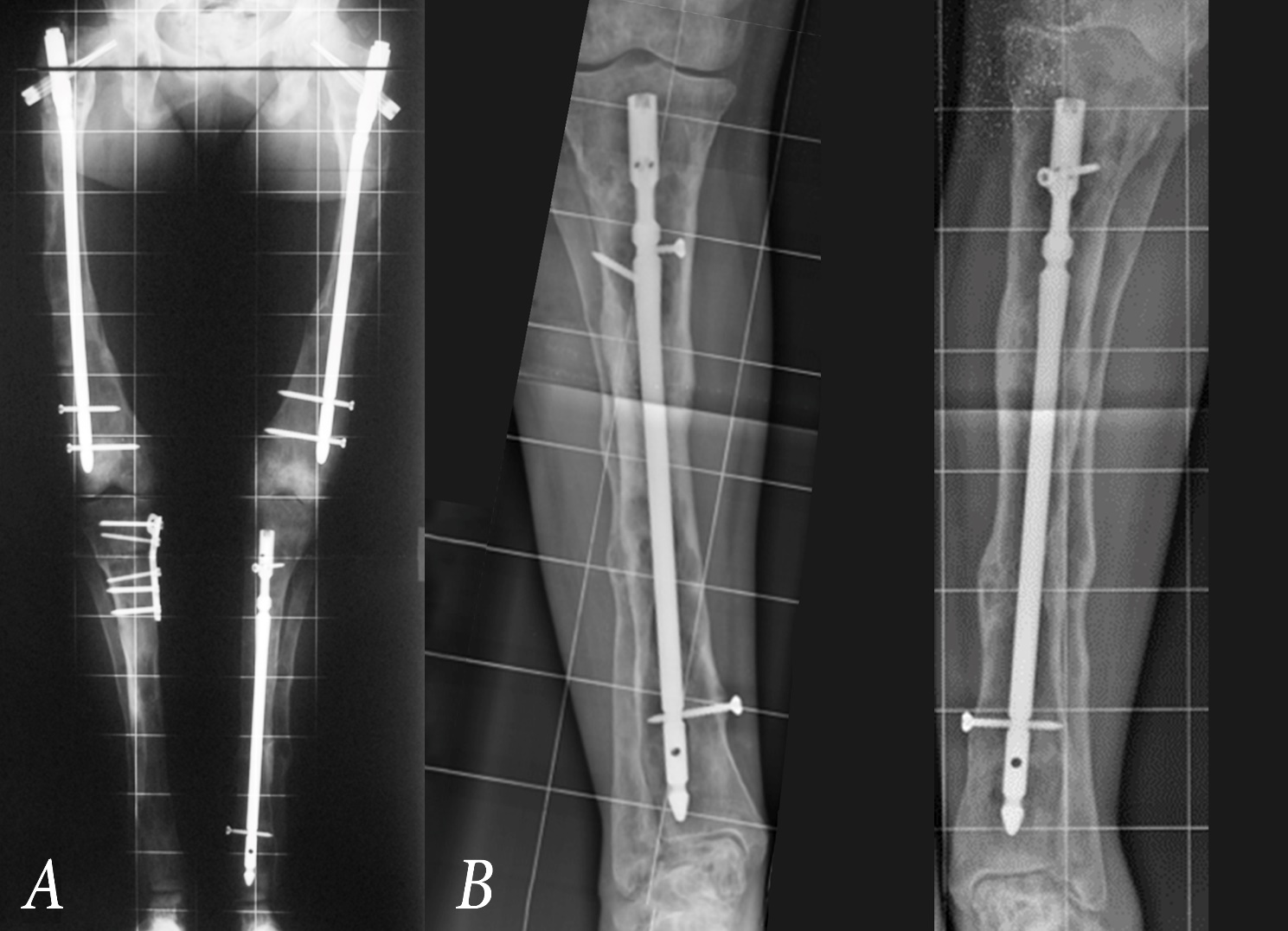
Regarding the surgical treatment of femoral deformities, we performed an additional osteotomy just distal to the intramedullary nail, close to the knee joint; the osteotomy line was oblique from lateral to medial until the proximal part of the medial femoral condyle; the triangular gap was filled by a synthetic triangular graft, while the osteotomy was stabilized using a screw plate (Fig. 1).the tibial osteotomy was performed to correct genu valgum secondary to tibial deformity, at the level of the proximal methaphysis. The osteotomy line was directed from the medial to the lateral side of the bone and stabilized by a screw plate. In both tibial osteotomies, the intramedullary nail was removed before surgery and reinserted after complete radiological healing of the osteotomy, at least 6 months after surgery (Fig. 2).


At follow-up, all patients were pain free, satisfied with the final correction obtained, without significant limitation of daily or social activities. Regarding the range of motion of the knee, we observed a full extension of the joint in all cases, while flexion ranged from 90° to 140°. Two patients showed mild limping unrelated to the alignment of the knee; one caused by a residual 3 cm lower limb inequality and the other due to hip muscles weakness. Femoro-tibial angle was corrected in all cases and it ranged from 0° to 8°. All the osteotomies healed within 4 months of the operation. No failure of the fixation implant was observed in any case.
DISCUSSION
The proximal part of the femur is frequently affected in PFD; coxa vara and shepherd’s crook deformity represent the most common deformities and may worsen over time, causing fractures, pain and limping. Treatment of these deformities is challenging, and it is generally based on single or multiple osteotomies stabilized by intramedullary cervico-diaphyseal rigid nails, as first described by Freeman et al in 1987.21 In some cases, blade plate or screw plate may be necessary, but they should be later converted in intramedullary devices when possible.
Some patients affected by PFD may present a genu valgum caused by a juxtaarticular deformity of the distal part of the femur or of the proximal part of the tibia. In some cases, valgus deformity of the knee occurs after surgical correction of the coxa vara and shepherd’s crook deformity.
The majority of the clinical studies regarding PFD are focused on the management of the main deformities of the proximal part of the femur, and do not report specific data on the juxtaarticular deformities of the knee.5,22–29 In 2015, Zhang et al10 reported some cases affected by PFD, stating that “valgus deformity in the iuxta-articular area may be secondary to surgical correction of the varus deformity in the proximal femoral shaft”. In these cases, when the femoro-tibial angle measured more than 10°, they suggested a varus supracondylar osteotomy stabilized by a screw plate. They also stated that this is the first report on the correction of the secondary genu valgum deformity in patients with PFD.
We operated on five patients affected by PFD or MAS with genu valgum greater than 15°, performing a femoral or tibial varus osteotomy stabilized with a screw-plate. In all cases, we obtained a good realignment of the affected limb, with a mild limitation of the knee flexion and mild limping in two cases. The osteotomies healed without significant complications, such as delayed unions, nonunions or infections.30
In agreement with other authors,10 we believe that genu valgum may occur in patients with PFD after a good correction of the main femoral and tibial deformities, caused by residual deformities of the distal femur or proximal tibial not realigned with intramedullary nail. In femoral deformities, the osteotomy and the internal fixation of the screw plate may be performed with the nail in site, while in tibial osteotomies the nail should be removed and reinserted after osteotomy healing.
The main limitations of the study are that it is retrospective, with a limited number of cases, without a control group and statistical analysis.
CONCLUSION
In conclusion, we believe that residual valgus deformities of the lower limb greater than 15 degrees should be corrected with additional surgery to improve function and cosmetic appearance of these patients. The osteotomy of the distal femur or of the proximal tibia represent the treatment of choice for the correction of this deformity, although in tibial osteotomies the surgical procedure cannot be performed in the presence of the intramedullary nail.
List of authors and their individual contributions
Gorgolini G (MD), (study design, manuscript preparation and editing)
Caterini A (MD), (data analysis, manuscript preparation)
Efremov K (MD), (data collection, manuscript preparation)
Marsiolo M (MD), (data analysis, manuscript preparation)
De Maio F (MD), (data analysis, manuscript preparation)
Farsetti P (MD), (study design, manuscript preparation)
Disclaimers
The Authors did not receive any funding or financial support or potential sources of conflict of interest.
The study have been performed in accordance with the ethical standards in the 1964 Declaration of Helsinki.