




INTRODUCTION
Osteochondritis dissecans (OCD) of the knee is an idiopathic, focal, acquired condition involving the osteochondral unit (subchondral bone and articular cartilage complex) having the potential to cause instability and separation of the osteochondral fragment from the joint surface which may results in intra-articular loose body formation and premature osteoarthritis.1–3
Historically the term osteochondritis dissecans was described in 1887 by König, who hypothesized an inflammatory genesis at the interface between cartilage and subchondral bone, but subsequent studies have disproved this hypothesis and the exact pathophysiology remains unclear at present.
More recently the OCD has been redefined by The Research on Osteochondritis Dissecans of the Knee (ROCK) group as a “focal, idiopathic alteration of subchondral bone with risk for instability and disruption of adjacent articular cartilage that may result in premature osteoarthritis”.4
The nature of OCD remains unclear, although several pathophysiology hypotheses have been proposed.5
According to the most recent literature, the etiology appears to be multifactorial and includes “biological factors” (eg. genetic predisposition, deficiency of ossification centers, disorders in blood supply and endocrine disorders such as vitamin D deficiency) and “mechanical factors” (eg. repetitive microtrauma, discoid meniscus, meniscus anterior horn instability, anterior tibial spine impingment).6–9 These factors would act synergistically in determining OCD.
OCD of the knee can be classified in two forms, according on skeletal maturity (open or closed growth plate status):
-
Juvenile OCD (JOCD)10
-
Adult OCD (AOCD)
The crucial difference is that the adult form (AOCD) rarely heals without surgery and has a poor prognosis, while the juvenile form (JOCD) has a better overall prognosis but it can require surgical treatment in case of unstable lesion or failure of conservative treatment.11
EPIDEMIOLOGY AND PATHOPHYSIOLOGY
The incidence of JOCD of the knee ranges from 2.3 to 31.6 cases out of 100.000,2,12 with an increasing incidence due to greater use of MRI and arthroscopy in the pediatric population, early competitive activity and intensive training. It mainly affects young males, with a male-to-female ratio of 5:3, mainly between the ages of 11 and 20.6,12
The knee anatomical site most frequently affected by JOCD is the posterolateral portion of the medial femoral condyle (over 70%), followed by the central portion of the lateral femoral condyle (15-20%), the inferior pole of the patella (5-10%) and the trochlea and tibial plateau (<1%).13 Bilateral JOCD varies from 14 to 30%.14,15
The microtraumatic theory of OCD is the one with the highest level of evidence.7,16 The initial factor is the impingment between the medial femoral condyle and anterior tibial spine. Fairbanks17 in 1933 was the first author who proposed traumatic theory as the cause of OCD. Subsequent studies have demonstrated the idea of the repetitive trauma or microtrauma, especially during sports as one of the principal underlying cause of OCD.18
Other factors implicated in this theory are obesity, lower limb alignment abnormalities, soft tissue insufficiency and anatomical variants such as discoid meniscus,19 greater posterior and medial tibial slope,20 smaller intercondylar notch21 and more distal location of posterior cruciate ligament.22
Other theories proposed are local ischemia: in fact, the subchondral bone has a vascularization susceptible to ischemia that is responsible of bone necrosis.23 Endocrine theories see vitamin D deficiency implicated in the etiopathogenesis of OCD.24,25 Some authors have suggested a familial inheritance in the etiology of OCD with reports of familial case and increased incidence in monozygotic twins, suggesting implication of genetic loci involved in cartilage turnover.26,27
Ultimately, the microtraumatic theory plays a central role in the etiopathogenesis of the OCD, despite being a multifactorial pathology.
CLINICAL PRESENTATIONS AND IMAGING
Patients affected by JOCD often presents poorly localized, activity-related knee pain. Weight bearing pain is the predominant symptom present in 80% of case, bus the symptoms are variable and will depend on the location and severity of the disease. Patients may also complain of joint swelling or locking, typical of unstable lesions or detached fragments.
JOCD can occur mainly in three clinical forms:
-
Accidental finding in an asymptomatic individual;
-
Mechanical pain during sports (most common form);
-
Continuous mechanical pain with joint swelling and/or locking
There are no pathognomonic or specific symptoms or signs of JOCD. The physical examination should include the hip (which can commonly refer pain to the knee) and the inspection of contralateral knee to exclude a bilateral form of OCD.
There is just one clinical test described by Wilson28 to identify JOCD only of the medial femoral condyle, although has a limited diagnostic value.29 It consists in flexing the knee from 0° to 90°, and passively extending the knee by internally rotating the foot. The test is considered positive if pain is elicited by internal rotation of the tibia during 30° to 90° of flexion and this pain disappears with external rotation of the foot.
Standard X-ray of the knee is the first diagnostic imaging test, to be performed in the AP, LL and tunnel view. Since the OCD is bilateral in about 15% of cases, it is necessary to perform radiographs of both knees. Typical radiographic appearance is a circumscribed area of subchondral bone separated by a sclerotic and radiolucent outline of the fragment. Radiographs are useful in diagnosis and for monitoring the lesion’s healing but with them it is not possible to assess the viability of the fragment and the subchondral bone-cartilage interface. Also, it’s not useful to predict the stability of the fragment.
Magnetic resonance imaging (MRI) is the examination of choice in the OCD as well as in diagnosis and for monitoring the lesion. It is able to confirm the radiographic diagnosis by viewing the fragment, which is usually hypo-intense on T1 images and characterized by a heterogeneous signal on T2 images; it also provides a better assessment of the size, the presence of bone edema or cystic lesions surrounding the lesion, the presence of a high signal intensity zone below the fragment or the presence of an intra-articular loose body. MRI has high diagnostic sensitivity, but poor accuracy to predict the stability of the fragment.10,22,30–34
CLASSIFICATION AND PROGNOSTIC FACTORS
During the time have been described several classification systems for OCD, based on radiographs, MRIs and arthroscopic findings (Table I).
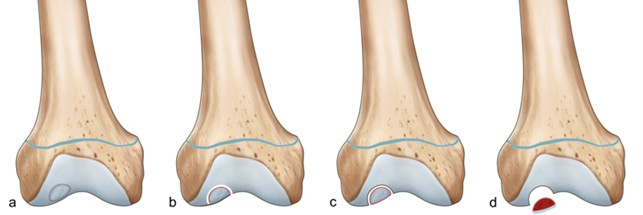
Berndt and Harty35 described 4 stages of OCD on plain radiographs (Figure 1):
-
Stage 1: small area, compression subchondral bone
-
Stage 2: partially detached OCD fragment
-
Stage 3: fully detached OCD fragment, still in underlying crater
-
Stage 4: complete detachment / loose body

Dipaola et al. suggested a classification based on MRI with arthroscopy findings correlations36:
-
Type I: thickening of articular cartilage and low signal changes, but no break
-
Type II: articular cartilage breached; low-signal rim behind fragment indicating fibrous attachment
-
Type III: articular cartilage breached; high signal changes behind fragment indicating synovial fluid between fragment and under-lying subchondral bone
-
Type IV: loose body
Guhl37 described 4 stages of OCD based on arthroscopic findings:
-
Type I: softening and irregularity of cartilage but no fragment
-
Type II: breached articular cartilage, low signal rim behind fragment indicating attachment
-
Type III: definable fragment, partially attached but displaceable (flap lesion)
-
Type IV: loose body and defect of articular surface
More recently, the ROCK Study Group developed a new arthroscopic classification of OCD of the knee divided in two main categories with three subgroups for each category38 with excellent intra and interobserver reliability:
-
Immobile OCD lesions:
-
Cue ball type (no abnormality)
-
Shadow type (cartilage is intact and subtly demarcated)
-
Wrinkle in the rug (cartilage is demarcated with a fissure, buckle and/or wrinkle)
-
-
Mobile OCD lesions:
-
Locked door (cartilage fissuring at periphery unable to hinge open)
-
Trapped door (cartilage fissuring at periphery able to hinge open)
-
Crater (exposed subchondral bone defect)
-
Regardless classifications of OCD, the most important aspect is the fragment stability that is the key factor governing prognosis and treatment decisions. The gold standard for the diagnosis of stability of the OCD lesion is the arthroscopic surgery, but it invasive and not amenable for all patient.
De Smet et al.10 defined some criteria of instability of the fragment evaluated on T2 images, among which, the presence of a hyperintense line behind the OCD fragment emerged as the most predictive criterion of instability and failure of conservative treatment (present in 72 % of cases) (Figure 2).

Also, Kijowski et al.39 showed 100% sensitivity and specificity for diagnosing OCD lesion instability if the following 3 signs were all present: a high T2 signal intensity rim surrounding a JOCD lesion of the same signal intensity as adjacent joint fluid, a secondary outer rim of low T2 signal intensity, and multiple breaks in the subchondral bone plate. Perilesional cysts were also found to be indicators of instability if they were either multiple or single but larger than 5 mm.
Despite MRI high diagnostic sensitivity (approximately 100%), it has poor accuracy to predict the stability of the fragment,10,22,30–34,40,41 especially in patients with open physes.39
Regarding prognostic factors, the age of the patient at the onset of symptoms is a factor that can significantly influence the prognosis. The onset of symptoms in adulthood is related to associated with worse outcomes than in skeletally immature patients13,42,43; in the latter group, age <12 years is associated with a more favorable prognosis. Another prognostic factor is the size of the lesion, with better results in patients with lesions <240 mm2.44
The prognosis also depends on site of the lesions: medial femoral condylar lesions has a good prognosis, instead patellar lesions have a poor prognosis, probably due to a higher rate of fragment instability.11
TREATMENT
OCD treatment has two main objectives: 1) to promote the healing of the subchondral bone and the overlying articular cartilage; 2) ensure joint congruity and to prevent the onset of early osteoarthritis.45
Conservative treatment, is the first line choice of management of JOCD of the knee, although there is no strong recommendation in the more recent AAOS guideline.11
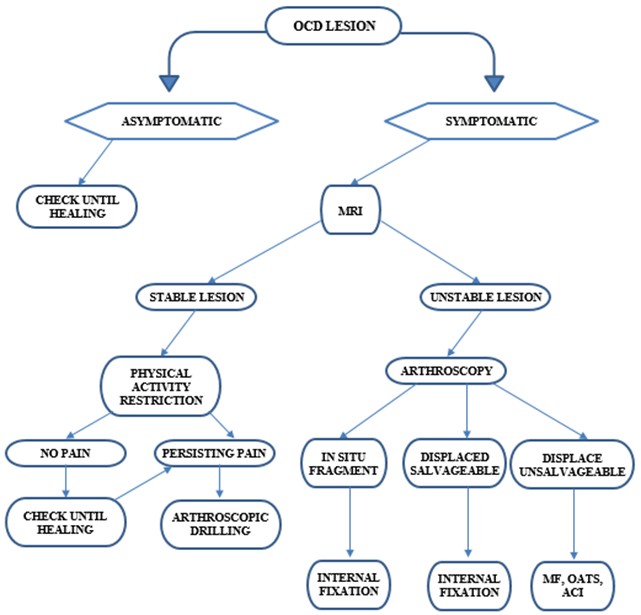
Treatment depends on stability of the lesion, age of the patient and symptoms. We also report our therapeutic algorithm in case of JOCD (Figure 3).

Conservative or nonsurgical, treatment has high rates of success in skeletally immature patients and should be the primary approach for stable JOCD of the knee.3,13,46
Non-operative treatment options include: immobilization (casting, bracing, splinting, unloader brace), limited weight-bearing and activity restriction.
When the diagnosis is incidental in an asymptomatic patient, it is sufficient to periodically check the patient until radiographic healing is achieved. In skeletally immature patients, who complain of knee pain and in whom the imaging findings document a stable lesion, conservative treatment continued for 3-6 months is the first-choice therapeutic strategy.
What emerges from a recent review of the literature is a lack of consensus on conservative treatment.3
The proposed non-surgical therapeutic options are represented by: physical activity restriction, physio kinesitherapy and muscle strengthening exercises, load restriction (partial with crutches or total with wheelchair), immobilization (with brace or plaster) and instrumental physical therapies, particularly in patients nearing the end of growth (eg. iontophoresis, shock waves and pulsed electromagnetic fields - PEMF’s).47 Among the various conservative treatments proposed, the restriction or suspension of physical activity (in particular activities involving pivoting, jumping and repetitive impacts) seems to be of primary importance.
Kocher et al.48 proposed a 3-step protocol for conservative management. Initially, immobilization and partial weight-bearing with crutches for 4-6 weeks. In the second phase, after radiographic control, weight-bearing without immobilization is permitted and the rehabilitation protocol begins with muscle strengthening and complete ROM recovery for another 6-12 weeks. If there are radiographic and clinical signs of healing at three to four months after the initial diagnosis, phase 3 can begin with gradual return to sport and a new control MRI is granted.
Persistent pain after 6 months and/or the development of signs of instability requires surgical treatment.
Surgical treatment is indicated after 6 months of conservative treatment with persistence or worsening of pain in the absence of signs of radiographic healing or in the event of signs of instability of the lesion on MRI.
There are several surgical techniques to be used depending on the type of injury: symptomatic and stable OCD lesion are managed by drilling. Unstable OCD lesion are managed by fixation of the fragment.
While, when the fragment has detached, salvage procedures are used.
Symptomatic stable OCD lesions, in which conservative treatment has not led to healing, are generally treated with arthroscopic assisted perforation of the subchondral bone with the aim of promoting healing at the subchondral cartilage-bone interface by promoting blood supply.
Two drilling techniques have been described: trans-articular or antegrade drilling and retro-articular or retrograde drilling.49–56
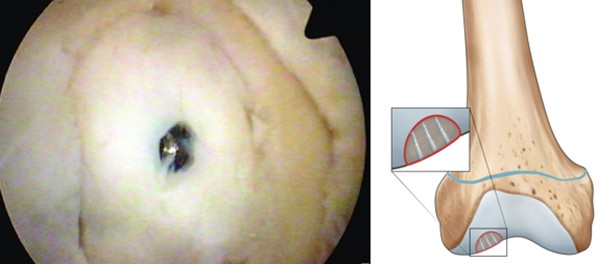
Trans-articular or antegrade drilling is performed during knee arthroscopy; several holes (5 to 10 depending on the lesion’s size) are drilled orthogonal to the articular cartilage of the OCD lesion with a 1.2-1.4 mm Kirschner wire until reaching the sub-chondral bone (approximately 20 mm deep). This technique is easy and rapid to perform but the disadvantages are that it violates the articular cartilage and far posterior condylar lesions may be difficult to access with this approach (Figure 4).

In retro-articular or retrograde drilling, holes are drilled in the subchondral epiphyseal bone under fluoroscopic guidance, from the outside to the inside of the knee, without entering the joint cavity and without violating the articular cartilage, while also sparing the metaphyseal growth plate of patients with cartilage metaphyseal still open. This is more technically demanding respect trans-articular approach because may be hard to locate and achieve accurate placement and depth of drills, requires a longer operative time and radiation exposure (Figure 5).

Trans-articular drilling technique is more frequently used,57 although a systematic literature review found no evidence that either method was better than the other.52
Outcomes of OCD drilling are favorable in most cases with high rates of healing and low complication rates.58
Unstable OCD lesions are generally treated with the fixation of the osteochondral fragment,56 with the main goal of preventing detachment or repositioning the detached fragment in the injury site to ensure joint congruity. Fixation is indicated for detached osteochondral fragments with normal macroscopic appearance of the articular cartilage and a layer of subchondral bone.
A variety of techniques have been described for fixation of unstable OCD lesions or detached fragments, such as fixation with resorbable implants (screws, anchors, arrows, pins)59–61 or metal implants (screws or pins),62,63 in combination with fibrin glue.
Regardless of the surgical technique (arthroscopic or open) or the type of fixation used, a fundamental step is represented by the preparation of the receiving “subchondral bed”, through an accurate cruentation for the removal of the fibrotic tissue and drilling to create vascular channels to maximize revascularization and increase the cure rate. If there is a resultant bone void, bone grafting from the proximal tibia or iliac crest is performed.
Generally, when the fragment has a discrete layer of subchondral bone, the choice of the fixation falls on metal screws because they guarantee good compression. The disadvantages are that metallic implants produce artifacts on MRI and often require second surgery to implant removal; also, metallic implant are associated with several complication such as migration, breakage and loosening (Figure 6).

Resorbable fixation devices, composed in polyglycolic acid (PGA) or polylactic acid (PLA), do not require removal, but in some cases resorption of the resorbable material may cause reactive synovitis associated with cystic lesions resulting in failure of synthesis64 (Figure 7).

The success rate has been reported between 91.7% and 100%57,65 with articular cartilage regeneration.64
Fixation of OCD fragment can be obtained biologically without the use of hardware, with autogenous osteochondral plugs collected from the non-weight-bearing part of the intercondylar notch.66–70
More recently, hybrid fixation has been proposed as an alternative method. It can be used when there is an unstable but partially salvageable OCD fragment, by combining mechanical compression screws (metallic or resorbable) and biological fixation (osteochondral autograft transplantation surgery (OATS)), with good or excellent outcomes.71–73
In some cases, fixation of the OCD lesion is not possible due to excessive fragmentation, incongruity of the donor site or cartilage wear. In these scenarios (rare in pediatric patients), the fragment is removed and the salvage techniques are used74: microfractures (MFX), autologous osteochondral transplants (OATS), fresh osteochondral allografts or autologous chondrocyte transplantation with ACI, MACI or AMIC techniques.
Microfracture drilling has been recommended for OCD lesions < 2 cm2,75 but it should be remembered that treatment with microfracture alone does not restore joint congruency and also in most OCD lesions this may not be possible as the subchondral bone is often absent. The outcomes are satisfactory in the short-term but deteriorate over time.76
For larger lesions, fresh osteochondral allograft transplantation procedures may be used. Advantages of this technique include the avoidance of donor-site morbidity and the ability to address large lesions with a single operation, but extensive serological, bacterial and viral testing of grafts is necessary prior to allograft transplantation.77,78 Also, immunological reactions against bony cells can be a cause of failure.79
Autologous chondrocyte implantation (ACI) or matrix-induced autologous chondrocyte implantation (MACI) has the same issue of not restoring congruity, although the bony defect can be dealt with using bone grafting. Several authors demonstrate favorable outcomes following ACI in patients with OCD of the knee80–84 (Figure 8).

CONCLUSIONS
Osteochondritis dissecans of the knee (OCD) is a multifactorial pathology in where repetitive microtrauma plays a central role in the etiopathogenesis. Conservative treatment with restricting sports activities is the first line treatment and often sufficient to ensure healing in patients with open physes. Surgical treatment depends on the persistence of symptoms after 6 months of conservative treatment and/or based on the development of signs of instability of the lesion.
List of authors and their individual contributions
Tudisco C (MD), (study design, manuscript preparation and editing)
Bernardi G (MD), (data analysis, manuscript preparation)
Maria Teresa M (MD), (data collection, manuscript preparation)
De Maio F (MD), (data analysis, manuscript preparation)
Gorgolini G (MD), (data analysis, manuscript preparation)
Farsetti P (MD), (study design, manuscript preparation)
Disclaimers
The Authors did not receive any funding or financial support or potential sources of conflict of interest.
The study have been performed in accordance with the ethical standards in the 1964 Declaration of Helsinki.