

INTRODUCTION
Revision total hip arthroplasty (THA) is a challenging procedure associated with inferior outcomes when compared with primary THA.1,2 Following revision THA, the most common causes of failure are aseptic loosening and instability.3 These complications are likely to be more frequent as the number of revision THA increases over the next decade.4 Large diameter head (LDH) prostheses offer a valuable option for tackling the risk of instability as they have been demonstrated to decrease the incidence of instability after revision THA.5
LDH THA can be defined as femoral head diameter ≥36 mm or wall thickness of the acetabular cup ≤12mm. Different designs of LDH THA exist, such as LDH ceramic-on-ceramic (CoC), LDH metal-on-metal (MoM) and dual mobility (DM) articulation. To maximise the bearing diameter, the wall thickness of the acetabular cup is kept minimal. Therefore, acetabular components of LDH THA are offered as a monobloc design or factory preassembled for CoC LDH. The primary stability of these components relies only on press-fit, as no supplementary screw fixation is possible.
The primary objective of this study is to assess the mid-term aseptic loosening rate of LDH monobloc press-fit components following revision THA. Secondary objectives are to evaluate complications by cause, assess for radiological evidence of implant failure, and measure patient-reported outcomes (PROMs). The hypothesis of this study is that LDH monobloc components implanted during revision THA offer satisfactory survival rate and clinical outcomes.
MATERIALS AND METHODS
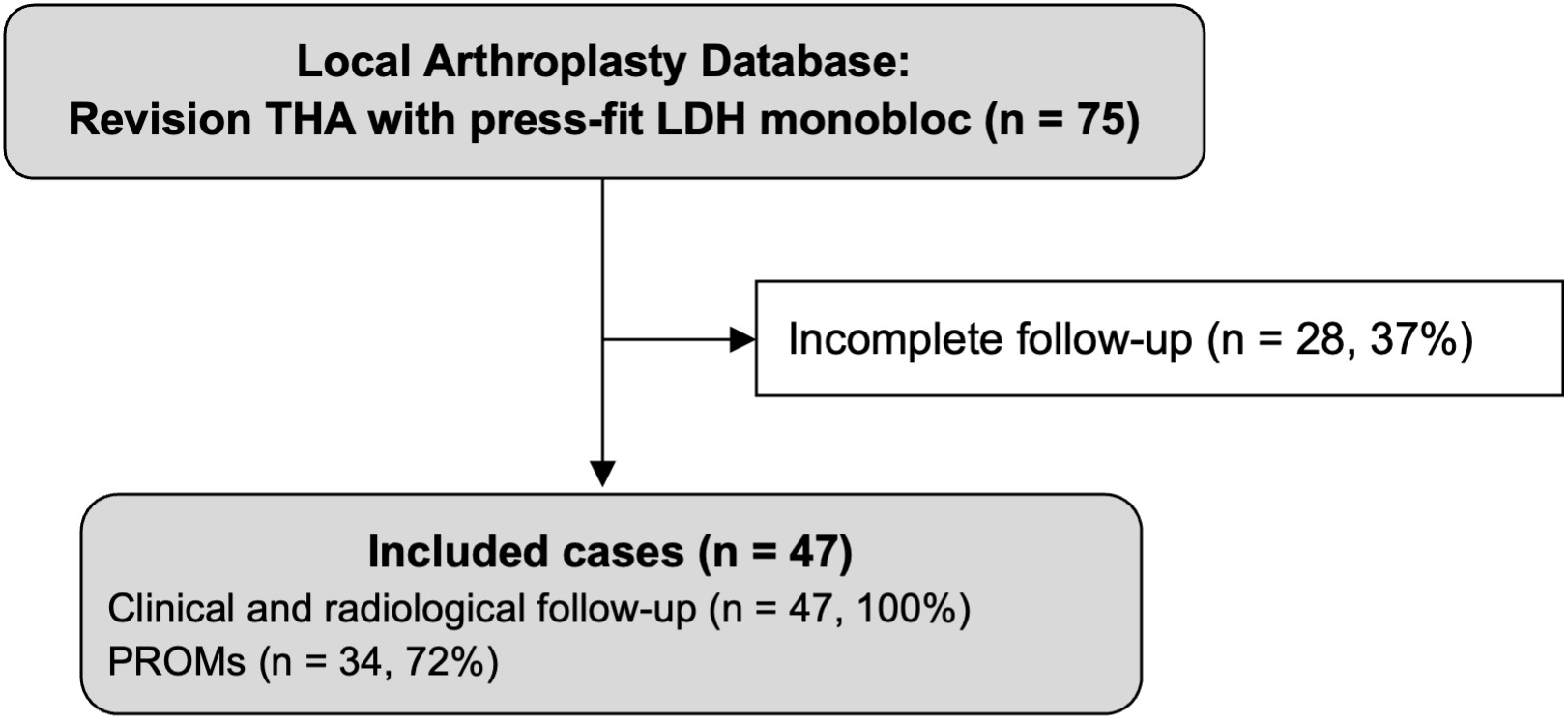
For this consecutive single-centre case series, the local arthroplasty database was used to retrospectively identify revision THA using press-fit only LDH monobloc acetabular components between 2007 and 2019. Inclusion criteria were a minimum follow-up of 2 years after revision THA and the availability of preoperative, postoperative, and last follow-up hip radiographs (Figure 1). Patients’ characteristics are summarized in Table 1.
Medical files were reviewed to gather perioperative data and identify complications during follow-up. Acetabular bone defects during revision THA were described according to the Paprosky classification.6 Revision failures for any cause were recorded. A radiographic evaluation on postoperative and last follow-up radiographs was conducted to identify signs of aseptic loosening of the acetabular component. Such signs included the presence of periacetabular radiolucent lines described with de DeLee and Charnley classification7 of more than 2 mm or acetabular component migration assessed using the technique described by Massin et al.8 Significant horizontal or vertical migration was defined as >3 mm,9 and significant variation of the acetabular inclination was defined as >5°.8 Post-revision radiographs were also assessed for heterotopic ossification described according to the Brooker classification,10 the presence of acetabular protrusion11 and superolateral acetabular uncoverage estimated by the technique described by Li et al.12 Functional outcomes were assessed at the last follow-up with the Western Ontario McMaster Universities Osteoarthritis Index (WOMAC, the best score is 0),13 the Forgotten Joint Score (FJS, the best score is 100),14 and the Patient’s Joint Perception question (PJP).15
Ethical Considerations
The study was conducted in accordance with the Declaration of Helsinki. The patient’s written consent was obtained, and ethical approval was received by the Institutional Ethics Committee of CIUSSS de l’Est-de-l’Île-de-Montréal (2021-2469; 01-2021).
Statistics
Continuous variables were described using means, standard deviations, and ranges. Categorical variables were defined using absolute and relative frequencies. Implant survivorship analyses were conducted using the Kaplan-Meier method and reported with a 95% confidence interval (CI), with acetabular component re-revision as the endpoint.16 Statistical analysis was performed using SPSS version 27 (IBM Corporation, Armonk, NY, USA).
Surgical technique
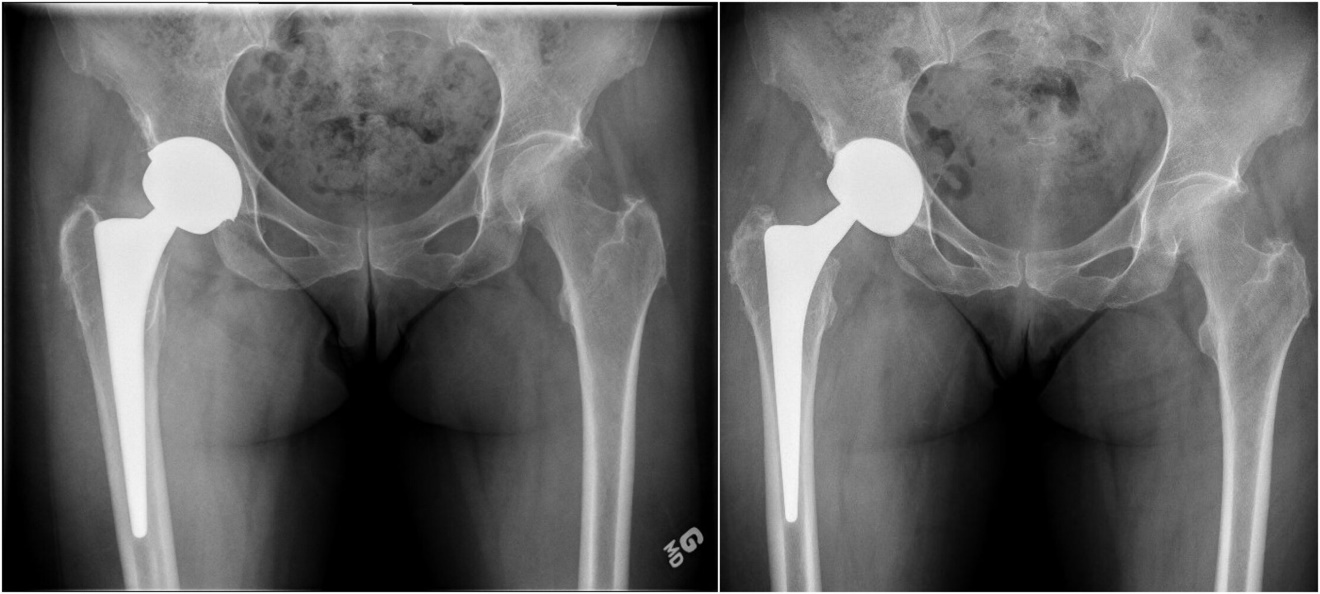
The procedures were performed by five experienced arthroplasty surgeons in our academic institutions. All revision THAs were performed using a posterior approach. The revision was limited to the acetabular component in 26 hips (55%). To retrieve the primary femoral stem, a femoral osteotomy was required in 3 cases (6%). To limit acetabular host bone deficits, the Explant (Zimmer Biomet, Warsaw, Indiana) was used to retrieve the acetabular cup. Allografts were used in 16 cases (34%) to augment acetabular deficits. Press-fit fixation of the acetabular component was obtained by 1 to 2 mm under reaming versus the implant’s outside diameter. Press-fit between the anterior and posterior acetabular rims was achieved in cases where a superior rim deficit was present. One such technique to achieve this was to medialize the implant to increase anterior and posterior rim contact. If superior contact was the preferred option where smaller defects were present; the center of rotation for the hip was elevated by 10 mm. Examples of these principles are demonstrated in Figure 2 and Figure 3.
_pelvis_radiograph_of_a_woman_of_39_years_of_age_who_had_a_tha_with_22.jpeg)

RESULTS
After an average follow-up of 4.5 years (2.7; 2.0 to 13.7), no aseptic loosening of the acetabular component was observed. Implant survivorship for any revision, at 4-years was 89.4% (95% CI: 89.3 to 89.5). There were 5 re-revisions (10.6%): 2 (4.3%) for loss of primary fixation (≤ 6 weeks) and 3 (6.4%) for instability, two of whom were primarily revised for instability. There was 1 (2.1%) non-revision reoperation for plate removal and femoral allograft in a patient with residual pain in whose revision THA had required femoral osteotomy which had been managed with a hook plate fixated with cerclage cables.
Regarding complications that did not require reoperation, there was 1 (2.1%) excessive postoperative blood loss that necessitated hospitalisation and transfusion, 1 (2.1%) peroperative acetabular fracture that was managed with six-weeks protective weight-bearing and remains stable six years post-revision, 1 (2.1%) pseudotumor secondary to metal debris of a MoM LDH prosthesis that was confirmed on magnetic resonance imaging (MRI) and managed conservatively, and 1 (2.1%) recurrent hip dislocation that remains under conservative treatment 6 years after the last event.
Last follow-up radiographic analyses revealed no additional signs of acetabular component aseptic loosening. The mean acetabular component abduction angle post-revision surgery was 43.1° (5.8°; 30.2° to 59.0°). Acetabular protrusion was present in 20 hips (42.6%), including 5 cases with pre-revision acetabular protrusion. The uncovered proportion of the acetabular component was 0 to 5% in 25 hips (53.2%), 6 to 10% in 8 hips (17.0%), 11 to 15% in 10 hips (21.3%), 16 to 20% in 3 hips (6.4%) and 21 to 25% in 1 hip (2.1%). At last follow-up, heterotopic ossification was categorized as Brooker class I for 8 hips (17.0%), class II for 1 hip (2.1%) and class III for 1 hip (2.1%). PROMs results are reported in Table 2.
DISCUSSION
There has been an increase in revision hip surgery over the last decade as the number of primary THA procedures has increased. Based on the UK joint registry alone, there has been an increase from 2730 in 2004 to 8087 in 2019.17 Revision surgery results in a less favourable quality of life; a paper by Lubbeke et al. indicates both Harris Hip Score (HHS) and WOMAC scores are significantly less for revision THA when compared with primary THA.18 The most common causes for revision of primary THA include instability, infection, and aseptic loosening.19,20 There is strong evidence in the literature that patient factors (such as age, gender, co-morbidities), surgeon experience and implant factors all impact the risk of revision.21–26
At our institution, the preferred option is an LDH using either monobloc or DM configuration for the acetabular component in primary THA and revision THA (Paprosky 1 and 2). There are numerous advantages to LDH implants. LDH THA offers an impingement-free range of motion and a reduced risk of dislocation.27–31 The larger head-neck offset allows for a greater supraphysiologic range of motion. This can also compensate for a patient’s abnormal spinopelvic mobility and surgical imprecision.32–34 Additionally, LDH bearing with a small clearance exerts a high suction force, which provides greater hip micro-stability.35,36 With appropriate biomechanical reconstruction, LDH THA can restore normal gait parameters.15,37,38 This results in unrestricted activities and higher patient satisfaction scores.15,38 We use CoC LDH for our patients with a life expectancy of more than 20 years and use DM bearings for all others.
Monobloc acetabular components do not allow for supplemental screw fixation, thus relying on press-fit for primary fixation. Compared to modular cups, monobloc components have not been associated with an increased rate of acetabular cup migration, aseptic loosening, or revision.39,40 Monobloc components offer optimal liner-shell conformity and eliminates liner-shell micromotion which has been proposed to reduce the risk of backside wear.41 Additionally, the absence of screw holes eliminates the access channels of wear debris to the subchondral bone, reducing the risk of acetabular osteolysis.42 Monobloc acetabular components in revision THA have been associated with favourable outcomes i.e., low aseptic loosening rates, significant improvement in functional outcomes and low re-revision rates.43,44
In our case series, using LDH cups for revision surgery, we found that implant survivorship at 4-years was 89.4% (95% CI: 89.3 to 89.5), wish is slightly superior to the 5-year survivorship of revision THA of 86.8% reported in the literature.21 After an average follow-up of 4.5 years (2.7; 2.0 to 13.7), no aseptic loosening of the acetabular component was observed. The reason for the 5 (10.6%) re-revisions varied and included: 2 loss of primary fixation (≤ 6 weeks) and 3 instabilities, 2 of whom were primarily revised for instability which have been associated with a higher risk of revision failure for instability.28 The third case of re-revision for instability was a revision of a MoM prosthesis which have been associated with higher complication rates, namely instability.45 Additionally, 2 of the failed revision for instability had a LDH prosthesis implanted during primary THA, which mitigates the advantages of using a LDH prosthesis for revision THA. Instability rates of up to 28% following revision THA have been reported in the literature, which are much higher than the instability rate of 8.5% reported in this series.46 Secondary outcome measures based on radiological imaging found no evidence of acetabular cup aseptic loosening.
The available literature supports these findings. A study by Klemt et al. using DM in revision THA with associated abductor deficiency demonstrated significantly lower dislocation rates at 4 years follow-up with 0% dislocations compared with 15.5% and 4.1% in conventional liners and constrained liners, respectively.47 Chalmers et al. found that LDH implants were a viable salvage option for high-risk cases with recurrent dislocation despite using constrained liners at a median follow up of 37 months.48 A study by Eckar et al. followed 216 patients for a median period of 69 months to assess the revision rate and dislocation rate of DM cups used in complex revision THA. The dislocation-free survival rate was 96% at 5 years and 82% at 9 years.49 A systematic review and meta-analysis performed by Pituckanotai et al. that reviewed 11 articles concluded that LDH is the implant of choice to reduce the risk of revision and dislocation when reviewing short term (0-5 year) outcome studies.50 LDH cups offer numerous advantages; the key advantage for revision is that it allows a larger area of contact between the cementless cup and the host’s bone.
The mode of fixation of the acetabular implant is widely discussed in the literature. For revision THA, the evidence in the literature suggests cemented fixation has been associated with poor outcomes and a high rate of loosening, whereas excellent outcomes have been documented with press-fit fixation in the revision THA.51–53 Our results also support that in revision THA with limited to moderate bone deficits that do not require structural allograft, adequate press-fit fixation of monobloc acetabular components can be obtained. An adequate press-fit on the anterior and posterior acetabular rims should be sought to optimize fixation. Therefore, if needed, the acetabular component should be medialized before attempting to increase the cup size. In cases of superior bone deficits, a high hip center of up to 10 mm can ensure adequate host bone contact on the superior dome, which is essential for the press-fit stability.54,55 While reaming, surgeons should use increments of 1 mm when approaching the desired diameter to ensure the sphericity of the reamed cavity. If desired, to gain confidence with press-fit only fixation, surgeons could seek adequate fixation with modular components without using screws before switching to press-fit monobloc acetabular components.
Khatod et al. investigated factors associated with re-revision and found the leading cause to be instability (42.9%), followed by infection (28.6%), and aseptic loosening (9.5%).21 Likewise, Springer et al. found instability to be the leading cause of re-revision (35%), followed by aseptic loosening (30%), and infection (12%).19 Interestingly, when reviewing the risk of re-revision, the evidence from the UK joint registry suggests a strong relationship between the time from primary THA to revision THA is a higher risk of re-revision. Causes for shorter time periods to revision would include instability as the leading cause, whereas more extended time periods to a revision include aseptic loosening.17 This is supported by Springer et al., whose research indicated that the survivorship of revisions at 10 years was 8.2%, with instability and aseptic loosening being the leading causes for the re-revision.19 It is stated that 20% of hips revised within a year of primary surgery are re-revised within 10 years; if primary hips lasted at least 5 years then the revision rate is 10.8% at 10 years.17
Implant survivorship is only one measure of success; it cannot be used to indicate satisfaction or improvement in function. While there is strong evidence in the literature supporting the use of LDH to improve functional range of motion in primary hips, there is limited data available for functional outcomes for the use of LDH in the revision setting. The benefits of using LDH in the primary setting includes a reduction in the risk of impingement (allowing for a greater range of movement and a decreased risk of dislocation); improved abductor function and hip kinematics; and a reduced long-term risk of implant loosening.56 Our study analysis functional outcomes for the use of LDH in the revision setting. This study demonstrates an improvement in functional outcomes when using LDH for revision surgery. The functional outcome scores highlighted include a WOMAC score of 19.5 (16.8; 0.0 to 58.3) and an FJS of 57.3 (28.9; 6.3 to 100.0); LDH for revision surgery is a good option. One of the few other studies that analyzes functional outcomes of LDH in the revision setting includes the study by Civinini et al. This study prospectively followed 33 patients for a mean of 3 years. The HHS improved from 48 preoperatively to 86 postoperatively, and the average total WOMAC score improved from 79 to 19 postoperatively.57
Limitations of the study
This study was performed in a tertiary centre with arthroplasty surgeons performing high volume complex revision THAs using monobloc LDH. This is not a true reflection of what is commonly practised. The results illustrated may not be replicated in all hospitals using the same implants if they were to adopt this technique. In addition, most acetabular defects were the type 1 Paprosky classification. The true extent of the application with other types of defects remains unclear. Finally, due to the retrospective nature of the study, cases planned for revision THA with a monobloc cup that were converted to a modular component intraoperatively were not included. The choice of implant type was based on the intraoperative judgment and technical abilities of the surgeon.
CONCLUSION
Based on our findings, the press-fit primary fixation of LDH monobloc components implanted in revision THAs is a safe and successful option. These acetabular components have demonstrated good mid-term results with low rates of relative complications while maintaining good functional outcomes.
ACKNOWLEDGEMENTS
We thank Dr. Alain Roy, Dr. Martin Lavigne, and Dr. Vincent Massé who contributed to the surgical procedures
AUTHOR CONTRIBUTIONS
Conceptualization, PAV, MWM and MOK.; methodology, PAS.; data acquisition and analysis, PAS and BB; writing - original draft preparation, PAS and SS; writing - review and editing, PAS, SS, BB, MWM, MOK and PAV; supervision, PAV and MOK. All authors have read and agreed to the published version of the manuscript.
DECLARATION OF CONFLICTING INTERESTS
PAV declares being a consultant for Stryker and Johnson & Johnson; receives royalties from Microport; and received research funding from Zimmer, Smith & Nephew, Johnson & Johnson, and Stryker. MOK declares he received research funding from Zimmer, Smith & Nephew, Johnson & Jonhson and Styker. PAS, SS and BB declare that they have no conflict of interest.
FUNDING
Unrestricted grant was obtained from the Maisonneuve-Rosemont hospital Foundation to support PAS Master’s degree University study tuition fees. The authors did not receive financial support for the research, authorship, and/or publication of this article.