.tif)
.tif)
INTRODUCTION
Clavicle fractures are estimated to account for up 2% to 10% of all fractures in adults, with 80% of them occurring in the middle third of the clavicle.1 Historically, middle-third fractures have been treated non-operatively, which consists of immobilization with a figure-of-eight brace or simple shoulder sling (Weeks 1 to 3), followed by gentle range of motion exercises (Weeks 3 to 6), and strengthening exercises (weeks 6 to 10).2 However, recent literature has identified higher nonunion rates (15-20%) and inferior functional outcomes in patients with non-operative management of displaced midshaft clavicular fractures when compared to those who underwent operative treatment.1,3–5 When compared to open reduction and internal fixation (ORIF), the Canadian Orthopaedic Trauma Society identified that operative patients had greater outcome scores, a shorter time to union (16.4 vs 28.4 weeks), lower rates of nonunion (3% vs. 14.2%), and lower rates of malunion (6.8% vs 0%).1 Similarly, a meta-analysis done by Zlowodzki et al.6 revealed that the relative risk for nonunion decreased by 86% when treated operatively versus nonoperatively.
Although there are many studies supporting the use of operative treatment,1,3,7 there are certain indications that need to be met. For instance, shortening greater than 1.5-2cm, displacement greater than 100%, a Z-shaped fracture pattern, evidence of neurovascular injury, open fracture, skin tenting, and a comminuted fracture.1,4 While operative treatment with ORIF has provided patients with superior outcomes and rates of union, there are still risks associated with surgical management that include reoperations (18%-25%) due to implant irritation, neuroma formation, and symptomatic malunion8,9
In this report, we present a patient who presented with a displaced, comminuted midshaft clavicle fracture following a fall while mountain biking. Despite the patient’s fracture meeting criteria for operative repair, the patient elected to undergo nonoperative management contrary to contemporary evidence-based medicine.
CASE PRESENTATION
A 58-year-old male with past medical history of paroxysmal atrial fibrillation and Lyme disease presented to the orthopaedic clinic with left shoulder pain that developed after being thrown over the handlebars of his mountain bike 8 days prior. Upon presentation to clinic, the patient rated his baseline pain a 3 on a scale of 1 to 10, with 10 being the worst. The patient endorsed a constant, throbbing and aching pain localized to left collar bone and extending laterally to his shoulder. Additionally, he stated that his pain was exacerbated by overhead movements (increasing to a 7-8 out of 10), application of any pressure to the region, and complete inability to lay on the injured shoulder.
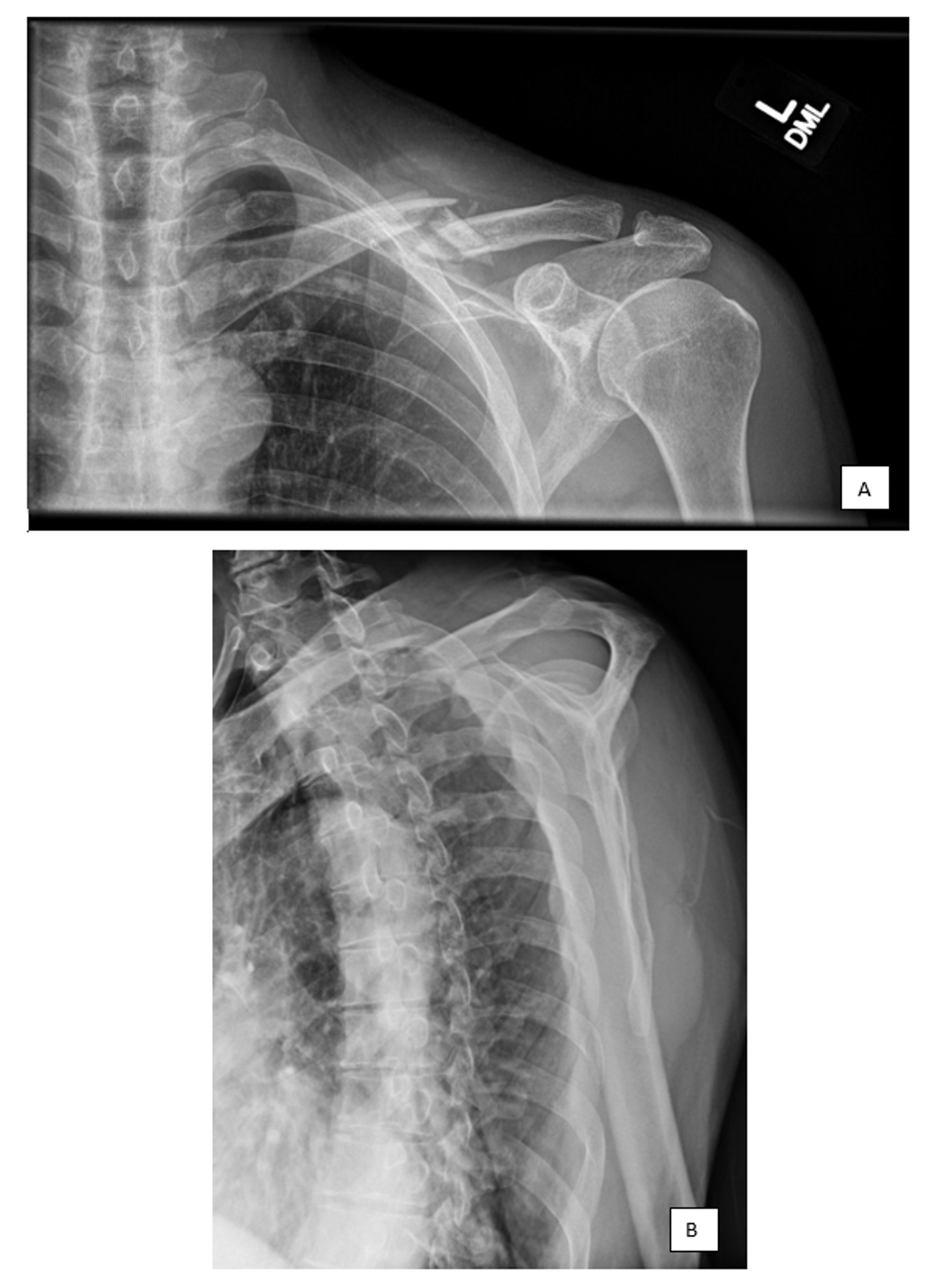
During the physical exam, noticeable deformity of the left clavicle region was noted - there was tenting of the overlying skin of the middle clavicle approximately 10-cm medial to the acromioclavicular joint as well as significant ecchymosis tracking from midshaft clavicle to the axilla. There was no evidence of an open fracture. There was tenderness to palpation over the middle clavicle of the patient’s injured left shoulder. Due to the degree of pain and discomfort, range of motion was not assessed for the affected side. However, the right shoulder displayed full range of motion (FF: 160, AB: 160). The patient was neurovascularly intact with preserved sensation across the C5-T1 dermatomes, intact distal motor function, and palpable distal pulses with a warm, well-perfused distal left extremity. Radiographs of the left extremity revealed an acute, displaced, comminuted midshaft clavicle fracture with associated overlying soft tissue edema. The X-ray also displayed nondisplaced fractures of the left fourth, fifth, and sixth ribs. There was no other evidence of fracture, dislocation, or osseous pathology to the patient’s left shoulder (Figure 1).
.png)
Given the patient’s age and fracture characteristics meeting criteria for surgical intervention, the patient was advised to undergo operative treatment to preserve long-term function and prevent continued symptomatology. Additionally, the risks and benefits of surgery were clearly outlined with the patient, and he was informed that his injury was at high risk for nonunion or malunion. However, the patient opted for nonoperative management due to subjective improvement in overall comfort, function, and pain, along with concern for his prior cardiac history. Thus, the treating physician (S.D.M) recommended nonoperative immobilization with a sling and over-the-counter analgesics for pain control. The patient was instructed to follow-up regularly in clinic to assess fracture healing and overall progression.
The patient followed up 1 week later, 15 days since injury, with repeat x-ray (Figure 2) and clinical evaluation. The patient reported no improvement in his overall discomfort and function, despite being compliant with sling immobilization. Pain continued to be rated as a 3 out of 10 with limited range of motion. Again, the patient’s physical examination was limited by pain and range of motion was not able to be assessed at this visit. The treating physician (S.D.M) recommended continued rest, ice, immobilization with a simple shoulder sling, and over the counter analgesics.
.tif)
Over the next three months, the patient was followed with regular clinic appointments and placed in a stepwise progressive nonoperative treatment program. Nonoperative management consisted of full-time immobilization in a simple shoulder sling with strict non-weight bearing for the first two weeks. After 2 to 3 weeks, the patient was permitted to use the affected arm with the elbow at the side for light activities. Following this, the patient was advised to advance his range of motion with gentle passive range of motion exercises followed by active-assisted and then active range of motion exercises for the following three weeks. During this period, he was advised to use his sling only for comfort. At six weeks, he was instructed to discontinue use of his sling and start gradual strengthening exercises with the aim of full return to function by three months.
At the patient’s three-month follow-up visit, radiographs illustrated a displaced, comminuted midshaft clavicle fracture with interval bony callus development along with multiple healing nondisplaced left sided rib fractures (Figure 3). Subjectively, the patient reported that he felt confident in resuming his previous active lifestyle with full strength and range-of-motion. Visual examination of the patient’s left shoulder demonstrated a gross deformity of the middle clavicle; however, it was nontender to palpation. Physical examination revealed painless, full range-of-motion equal to his contralateral, non-injured shoulder. Additionally, he had 5/5 strength equal to his contralateral, non-injured shoulder, along with negative rotator cuff exam maneuvers. As a result of the resolution of clinical symptoms and a return to full strength and function, the patient was recommended to follow-up as needed. Currently, the patient is over 18-months post-injury and remains satisfied with nonoperative outcome.
.tif)
DISCUSSION
There has been a significant amount of literature generated over the past decade addressing the optimal treatment strategy for treating displaced midshaft clavicle fractures in adults; however, there is yet to be a consensus. Surgical indications have expanded to now include open fractures, severe angulation, comminution, displacement, skin tenting with a threat of skin perforation, neurovascular compromise, symptomatic nonunion, and fracture shortening >1.5-2cm.10 Undergoing operative repair has demonstrated a faster time to union, greater patient reported outcome scores, and higher satisfaction compared to patients that are treated nonsurgically.3 Additionally, other studies have reported higher functional scores in surgically managed patients at 3 weeks post-op.11 Zlowodzki et al. reported that the nonunion rate for displaced midshaft clavicular fractures was 2.2% after plate fixation compared with 15.1% after nonoperative care, displaying a relative risk reduction for nonunion of 86%.6 Furthermore, operative fixation has been noted to eliminate a majority of the complications identified in nonoperative patients, such as the 15%-20% rate of nonunion, the 10%-20% rate of malunion, the 18%-33% loss of strength, and the presence of neurologic sequelae in up to 12% of patients.3–5,12
It is important to note that multiple studies have reported that nonoperative treatment demonstrates positive outcomes that match those of patients undergoing operative treatment. A systematic review by Virtanen et al.13 found that after 6 months the benefits of operative treatment were minimal compared to nonoperative treatment. Also, the nonoperative group was noted to have adequate functional results, pain relief, and union rates during this timeframe. Similarly, Ahrens et al.14 and Judd et al.11 identified that by 9 months there was no significant difference in patient reported outcomes/patient satisfaction (Disabilities of the Arm, Shoulder, and Hand score and Constant-Murley scores) between operative and nonoperative patients. Furthermore, in a combined series of over 3000 midclavicular fractures, there was a reported nonunion of 0.4% when treated nonoperatively.5
Alongside the published benefits and outcomes associated with nonoperative and surgical management of midshaft clavicle factures, there are also well-documented complications associated with each treatment strategy. Symptomatic nonunion and malunion of the clavicle are the two most common complications of nonsurgical management, with symptomatic nonunion occurring in 14% to 24% of patients.1 Common complications for surgical management include supraclavicular numbness from iatrogenic injury to branches of the supraclavicular nerve, superficial and deep infection, implant irritation, revision surgery, and nonunion.3 Overall, there is currently a heterogenous mixture of studies in the literature surrounding the best management for midshaft clavicle fractures.
The current study reports a patient that met surgical indications for traditional operative clavicle repair, but the patient refused surgical intervention and elected to pursue nonoperative management. Despite certain literature demonstrating that patients who received nonoperative management for their clavicle fracture demonstrated inferior outcomes and decreased strength compared to surgical treatment,4,5 this patient exhibited complete recovery to baseline strength and range-of-motion by 3-month follow-up. Furthermore, while nonoperative management of midshaft clavicle fractures is not uncommon, it is rare for patients with the aforementioned surgical indications to regain full strength and range of motion within three months from injury. We hypothesize that this patient’s stark improvement was secondary to his lack of significant concomitant injuries, rehabilitation compliance and active pre-injury lifestyle. In summation, the literature illustrates an ongoing debate of clavicle fracture management. As such, this case report adds to the discussion and provides evidence for the nonoperative management of displaced, comminuted midshaft clavicle fractures.
Acknowledgements
Conine Family Fund for Joint Preservation
Author Contributions (all authors meet the 4 criteria recommended by the ICMJE)
Sara A. Naessig, BA: Conceptualization, Design, Data curation, Formal Analysis, Investigation, Methodology, Validation, Writing- original draft, Writing- reviewing/revising/editing, Approval of final version, Acknowledges accountability for the accuracy and integrity of this work.
Christopher T. Eberlin, BS: Conceptualization, Design, Data curation, Formal Analysis, Investigation, Methodology, Validation, Writing- original draft, Writing- reviewing/revising/editing, Approval of final version, Acknowledges accountability for the accuracy and integrity of this work.
Michael P. Kucharik, MD: Conceptualization, Design, Data curation, Formal Analysis, Investigation, Methodology, Validation, Writing- original draft, Writing- reviewing/revising/editing, Approval of final version, Acknowledges accountability for the accuracy and integrity of this work.
Nathan J. Cherian, MD: Conceptualization, Design, Data curation, Formal Analysis, Investigation, Methodology, Validation, Writing- original draft, Writing- reviewing/revising/editing, Approval of final version, Acknowledges accountability for the accuracy and integrity of this work.
Scott D. Martin, MD: Conceptualization, Project Administration, Design, Data curation, Formal Analysis, Investigation, Methodology, Validation, Writing- original draft, Writing- reviewing/revising/editing, Supervision, Resource provisions, Approval of final version, Acknowledges accountability for the accuracy and integrity of this work.
Financial Disclosure Statement
All authors, their immediate families, and any research foundation(s) with which they are affiliated did not receive any financial payments or other benefits from any commercial entity related to the subject of this article – as of August 31, 2022