Introduction
Forearm fractures are common in childhood. Radius and ulna fractures account for 40% of all fractures that children experience with a greater incidence during the summer months. Ninety percent of all forearm fractures in youth occur outdoors, and dry weather increases the risk, as compared to rainy days.1 Distal fractures are also more common than proximal ones.2 Within distal fractures, the ulnar styloid is most commonly affected, representing 80% of all distal intraarticular radius injuries.3 Metaphyseal fractures of the ulna occur within 5 cm of the ulnar head dome, and these comprise 5% of distal radius fractures.4
Clinical signs of forearm fracture include perceptible deformity, tenderness, and reduced range of motion. Most often, it is the joint adjacent to the fracture that experiences the reduced mobility; usually the wrist for distal and the elbow for proximal fractures.2 In confirming the suspected diagnosis, evidence from radiographs is almost always used.
When falling, children instinctively protect themselves by extending their upper extremities to brace their landing. Most times, their pronated arms withstand most of the impact, forcing their forearms to bend dorsally into a supinated position, which often leads to injury.5
In many instances, clinicians may be unclear about the mechanism of an upper extremity fracture, especially a distal ulnar fracture. In these scenarios, there should be a high-level of suspicion of abuse, as these injuries have been linked to intimate partner violence.6 However, there has not been a significant correlation between patterns of distal ulnar fractures and child abuse.7
In the following case, we discuss a repeat forearm fracture experienced by a child during a regular school day and the treatment options to consider in such an event.
Case presentation
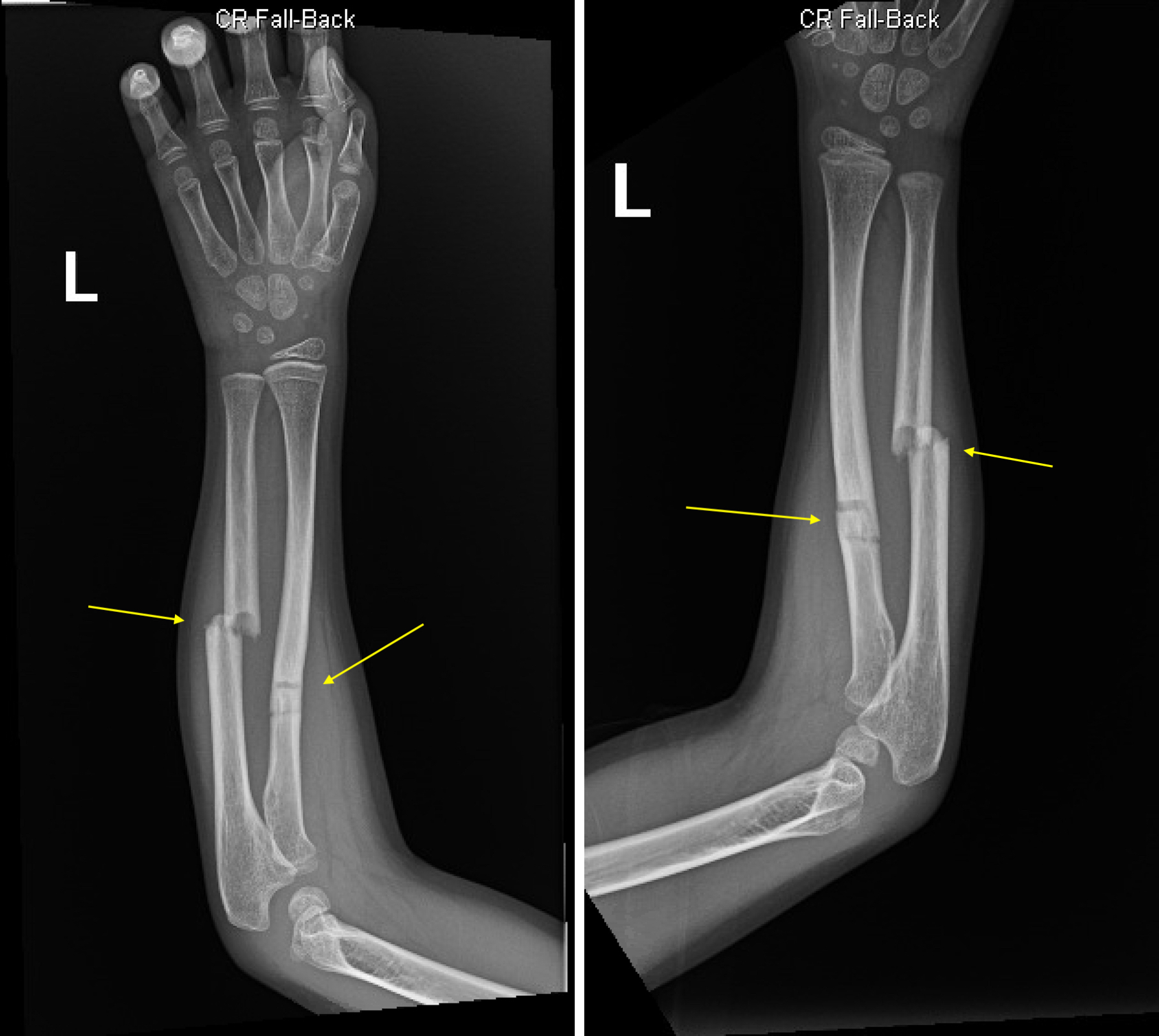
A 7 year old boy presented to the ED following a fall incident on the classroom carpet wherein he landed on his left arm. He arrived with a chief complaint of pain throughout his left arm. A physical exam revealed tenderness to palpation mid shaft and neurovasculature remained intact. Bone density was within normal limits, and the patient denied any fevers, chills, chest pain, shortness of breath, nausea, vomiting, diarrhea, abdominal pain, headache, or urinary symptoms. The patient had decreased conspicuity of the ulna and had a partial fracture of the mid radial diaphysis with 20-30% overriding of the fracture fragments. There was a mildly angulated fracture of the radius in the proximal/mid region. Two views of the fracture were obtained (figure 1).
_and_supinated_(right)_views_of_the_forearm_demonstrate_greenstick_fracture.jpg)
Three months earlier, the patient experienced an accident leading to greenstick fractures of the mid radial and ulnar diaphyses with volar angulation in his left arm. One month prior, the patient had come out of casting, wore a splint for approximately a week, and then allowed the arm to heal without any assistive devices. During the current visit, the patient was provided a full splint and prescribed 200 mg of ibuprofen.
The patient’s vital signs revealed a temperature of 97.7°F, a pulse of 103 beats per minute, a respiratory rate of 18 breaths per minute, a blood pressure of 103/66, and an oxygen saturation of 99% on room air. He did not have any significant surgical history.
After discharge, the patient followed-up with an Orthopedics physician for further management.
Discussion
When managing forearm fractures the ability to perform regular pronation and supination is a key element. The American Academy of Orthopedic Surgeons classifies normal pronation as 71 degrees and supination as 84 degrees.8 For severely displaced or angulated forearm fractures, reduction and immobilization are deemed necessary. Reduction requires knowledge of the injury mechanism. The main idea is to position the bone to its original state in the direction opposite of how the injury occurred. After reaching proper alignment of the bones, a long arm cast over the elbow is suggested.9 Casting helps limit mobilization and contraction of surrounding muscles. A study involving 48 patients with forearm fractures between 4 and 12 years of age were treated with closed reduction and casting during a two year period. In this cohort, 86% of patients had near-perfect functional outcomes and none had a poor recovery.10
Clear indications for surgical treatment include open fractures, segmental fractures, floating elbows, and fractures involving critical soft-tissue complications.5 Bowman et al. reports that the highest risk groups for surgery are patients above 10 years of age, individuals who have a proximal-third radius fracture, and those with an ulna fracture where the angle is less than 15 degrees.11
Up to 80% of all forearm fracture cases involving surgical intervention use elastic-stable intramedullary nailing (ESIN).12 ESIN describes a minimally invasive operation wherein two elastic nails are inserted through the metaphysis and into the medullary canal. A primary factor that determines the use of ESIN is the patient’s age. For preschool age, ESIN is highly unusual. However, it is most commonly used for children in grade-school to promote osteosynthesis.5
Long-term mobility and functionality following distal forearm fractures varies in pediatric populations. A study involving 220 pediatric cases with a median follow-up time of 10 years reports that 19% of patients continue to have pain in the injured wrist, 5% have decreased mobility, and 9% have moderate/poor overall recovery. It was found that patients above 10 years of age with fractures healed to an angular deformity of > 20% consistently demonstrated worse recoveries.13
Conclusion
Forearm fractures are a regular occurrence for young children. Physicians should inquire about the mechanism of injury to understand its etiology and to guide closed reduction of the injured bone. The goal is to restore mobility for the patient with proper pronation (71 degrees) and supination (84 degrees) as key objectives. When operative treatment is required, ESIN should be considered for patients as it is proven to yield successful outcomes. Casting helps immobilize the forearm until a full recovery is achieved.
Ethical considerations
HCA Centralized Algorithms for Research Rules on IRB Exemptions (CARRIE)/ IRB manager issued study exemption # 2022-819.
Disclaimer
This research was supported (in whole or in part) by HCA Healthcare and/or an HCA Healthcare affiliated entity. The views expressed in this publication represent those of the author(s) and do not necessarily represent the official views of HCA Healthcare or any of its affiliated entities.