
INTRODUCTION
Osteoporosis is a common chronic non-communicable disease with heterogenic management according to the different national approaches.1 The prevalence of osteoporosis is predicted to increase in the future due to the aging of the population.2 In 1994 World Health Organization (WHO) recognized osteoporosis as a well-defined disease and provided its diagnostic criteria based on the assessment of the BMD.3 BMD at the femoral neck was considered as a reference standard to define osteoporosis. Subjects with a BMD value 2.5 standard deviations (SD) or more below the young female adult mean (T-score less than or equal to –2.5 SD) are classified as “osteoporotic”.4
Osteoporosis is divided into primary and secondary forms. Primary osteoporosis occurs in postmenopausal women in relation to oestrogen deficiency and in senile people according to impaired calcium absorption in the intestine as a result of decreased levels of vitamin D3 and low activity. Secondary osteoporosis occurs due to underlying diseases and the use of some drugs. Endocrine, gastrointestinal, liver, hematological, rheumatological, renal, genetic, etc. diseases can cause osteoporosis. The use of medications such as glucocorticoids, anti-epileptics, chemotherapy agents, proton pump inhibitors, and thiazolidines are also related to osteoporosis.5,6
Low BMD and microarchitectural deterioration of the osteoporotic bone are associated with an increased risk of fragility fractures. Fragility fractures are fractures caused by mechanical forces that would not normally break a healthy bone, known as low-level (or ‘low energy’) trauma.6–8 20% of the patients who experienced one fracture are at risk for a second fracture within the first year. The costs of osteoporotic fractures in the European Union accounted for €32 billion in the year 2000 and were predicted to double by 2050.2
Risk factors for osteoporosis are fixed and modifiable. Fixed risk factors include age, height loss, female gender, family history of osteoporosis, previous fracture, ethnicity, estrogen deficiency, amenorrhea, menopause, and hysterectomy.9–12 Modifiable risk factors include alcohol consumption, smoking, low body mass index (BMI), poor nutrition, low dietary calcium intake, vitamin D deficiency, eating disorders, insufficient exercise, and frequent falls. Most of them impact bone biology and lead to a decrease in BMD, but some of them increase the risk of fracture independently.13,14
There are several tools for the assessment of osteoporotic and fracture risk. Currently, the most popular tool is the fracture risk assessment model FRAX published on the University of Sheffield website in 2008. The FRAX model provides a framework that improves fracture risk assessment in men and women, integrating clinical risk factors alone or in combination with BMD.15 FRAX has been developed to calculate the 10-year probability of major osteoporotic fracture or hip fracture.16 The aim of this study was to assess the prevalence of low BMD at axial sites and fracture risk in the Bulgarian population.
MATERIALS AND METHODS
Ethical considerations
All procedures performed were in accordance with the ethical standards of the institutional and/or national research committee.
Assessed parameters
We retrospectively assessed the DXA scan results of 12 478 subjects conducted between 2011 and 2019 in two sites in Pleven, Bulgaria - Diagnostic Consultative Center “Avis Medika” and Clinic of Imaging Diagnostics of the University Hospital “Dr. Georgi Stranski”. DXA osteodensitometry was performed with DEXA devices Lunar Prodigy made by General Electric and QDR 4500 C made by Hologic, USA.
Data were available for the following subjects’ characteristics: sex, age, weight, height, and BMI. Subjects were divided into age decades. Scan results included parameters for the lumbar spine and femur. The accessible lumbar spine variables were BMD and T-score of the whole spine. Hip assessments included information about BMD and T-score of the femoral neck. FRAX for MOF and FRAX for HF were assessed in subjects between 40 and 90 years with BMD. FRAX was calculated using the United Kingdom algorithm due to the absence of a national model in the time period between 2011 and 2019.
Definitions
T-score values were considered as normal if >-1 SD, osteopenic if ≤-1 and >-2.5 SD, and osteoporotic if ≤-2.5 SD. Each zone with an available T-score value was defined into three groups – normal, osteopenic, and osteoporotic. Subjects were attributed to three groups: 1st group - women aged 50 years and older, 2nd group - women under 50 years, and 3th group - male subjects. Subjects with BMI under 18,5 kg/m2 were considered underweight, those with BMI between 18.5 and 24.9 kg/m2 were considered to be normal weight and those with BMI equal or above 25 kg/m2 were defined as overweight.
Statistical analysis
SPSS 19.0 was used to assess the data. We summarized the collected information through descriptive statistics in tables with mean values, minimum, maximum values, standard deviations, and standard errors. Pearson’s chi-squared test was used to determine whether there is a statistically significant difference between the expected frequencies and the observed frequencies. Analysis of variance (ANOVA) was used to analyze the differences among two or more population means. Statistical significance was set as p≤0.05.
RESULTS
Of 12 478 subjects, 12 119 were women (10 420 women aged 50 yrs. or older and 1699 women under 50 yrs.) and 359 were men. The mean age of the subjects was 61 years (yrs.) ± 10 yrs. (range 18-93 yrs.), mean weight - 69.7 kilograms (kg.) ± 14.5 kg. (range 35-162 kg), mean height - 161 centimeters (cm) ± 7 cm (range 115-195 cm) and mean BMI was 26.9 kg/m2 ± 5.3 kg/m2 (range 13.7 kg/m2 - 65.8 kg/m2). Age, weight, height, and BMI differed significantly between the groups: females ≥50 yrs., females <50 yrs. and males with p-values corresponding to 0.000 for each subject’s characteristics, table 1.
7432/12 478 (59.6%) subjects were overweight, 4746/12 478 subjects (38%) were of normal weight and 301/12 478 subjects (2.4%) were underweight. In the group of the female subjects ≥50 yrs., 6 428/10 420 women (61.7%) were overweight, 3 792/10 420 women (36.4%) were of normal weight and 201/10 420 women (1.9%) were underweight. In the group of the female subjects <50 yrs., 807/1699 women (47.5%) were overweight, 3 792/1699 women (47.1%) were of normal weight and 92/1699 women (5.4%) were underweight. In the group of male subjects, 197/359 men (54.9%) were overweight, 154/359 men (42.9%) were with normal weight and 8/359 men (2.2%) were underweight, table 2. BMI categories differed significantly between the subjects’ groups, p=0.000.
Distribution of the subjects according to the age decades
Of total 10 420 female subjects - 3 574/ (34.3%) were aged 50-59 yrs., 4 093 (39.3%) were 60-69 yrs., 2 335 (22.4%) were 70-79 yrs., 409 (3,9%) were 80-89 yrs. and 9 (0.1%) were ≥90 yrs. Of overall 1699 women under 50 yrs., 12 (0.7%) were under 20 yrs., 26 (1.5%) were aged 20-29 yrs., 152 (8.9%) were 30-39 yrs. and 1 509 (88.8%) were 40-49 yrs. Of total 359 male subjects, 12 (3.3%) were 20-29 yrs., 26 (7.2%) were 30-39 yrs., 81 (22.6%) were 40-49 yrs., 74 (20.6%) were 50-59 yrs., 104 (29%) were 60-69 yrs., 49 (13.6%) were 70-79 yrs. and 13 (3.6%) were ≥80 yrs.
Bone mineral density
BMD and T-score values of the lumbar spine were assessed in 9 336/12 478 subjects (74.8%). BMD and T-score values of the femoral neck were present for 3 140/12 478 subjects (25.2%). The mean total BMD of the lumbar spine was 0.970 g/cm2±0.19 SD and the mean total T-score of the lumbar spine assessments was -1.24 SD±1.53 SD. The mean total BMD of the femoral neck was 0.797 g/cm2±.15 SD and the mean total T-score of the femoral neck was -1.30 SD±1.17 SD.
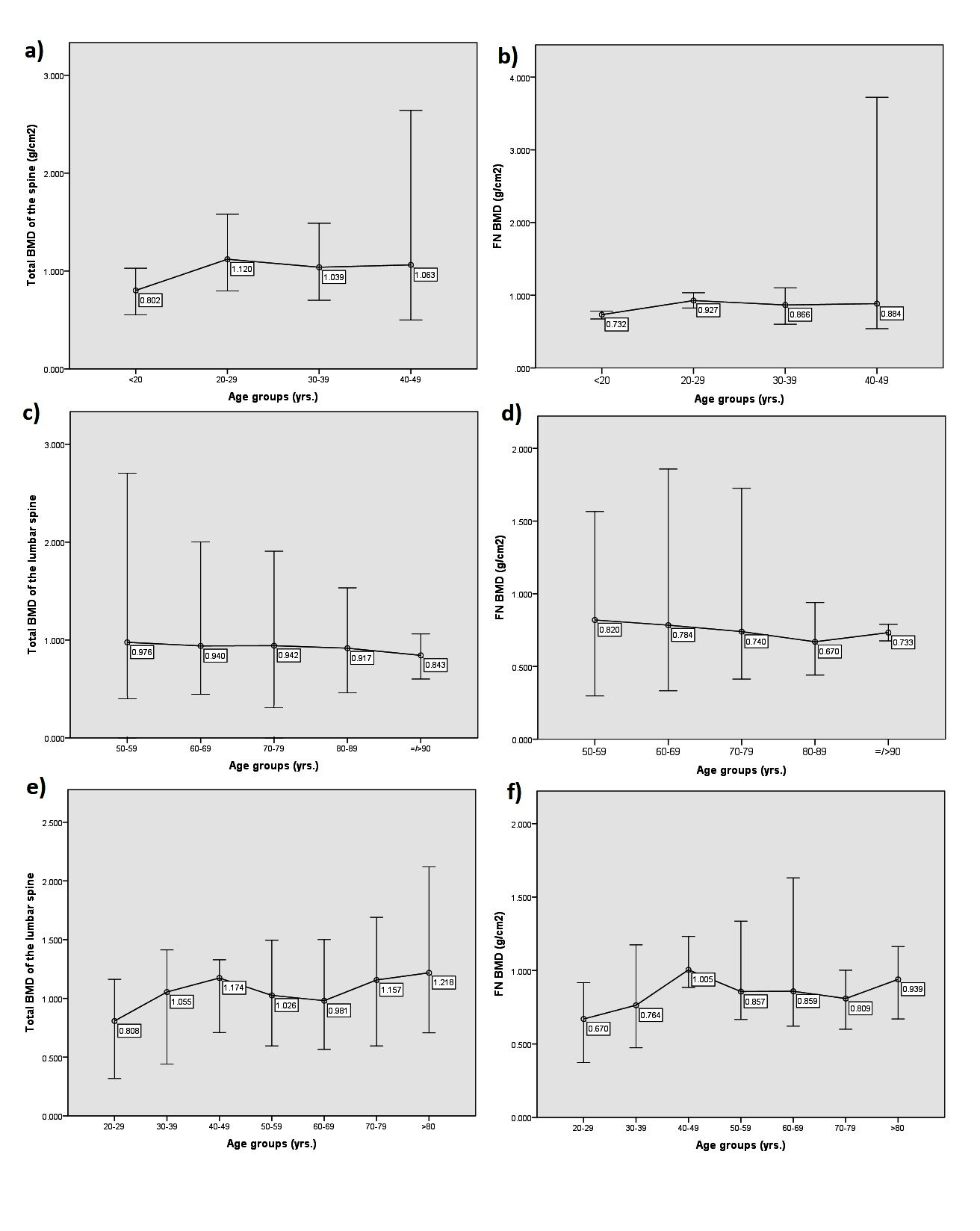
1 262 lumbar spine acquisitions and 432 femoral neck scans were done for female subjects <50 yrs. The mean total BMD values of the lumbar spine differed significantly between the groups according to the age decades (p=0.001). Interestingly, the youngest group is under 20 yrs. showed the lowest mean total BMD of the lumbar spine and the group with age interval 20-29 showed the highest mean total BMD of the lumbar spine, fig. 1a). Mean BMD values of the femoral neck didn’t differ significantly (p=0.342) between the age groups and decreased with the age excepting the age group 20-29 yrs. where the mean BMD of the femoral neck was the lowest compared to other age groups, fig. 1b).
_mean_bmd_of_the_total_lumbar.jpeg)
Women aged 50 and older had 7 803 lumbar spine scans and 2 611 femoral neck scans. The mean total BMD values of the lumbar spine and the mean BMD values of the femoral neck differed significantly between the age decades (p=0.000 for both groups). The mean total BMD of the lumbar spine decreased with increasing age decade, fig.1c). The mean BMD of the femoral neck also decreased with increasing the age decade except for the age decade ≥90 yrs. where the mean BMD was higher compared to the age decade 80-89 yrs., fig.1d).
264 men had assessments for total BMD of the lumbar spine and 95 men had results for femoral neck BMD. The mean total BMD of the lumbar spine differed significantly in the different decades of age in male subjects (p=0.000). The mean BMD values of the femoral neck didn’t differ significantly in the different decades of age in male subjects (p=0.07). It can be seen that the age groups 20-29 yrs. and 30-39 showed lower mean total BMD of the lumbar spine and mean BMD of the femoral neck compared to other age groups. In men over 50 yrs., the lowest mean total BMD of the lumbar spine was present in the age group 60-69 yrs. and the lowest mean BMD of the femoral neck was present in the age group 70-79 yrs, fig.1e), fig.1f).
Prevalence of low BMD at axial sites
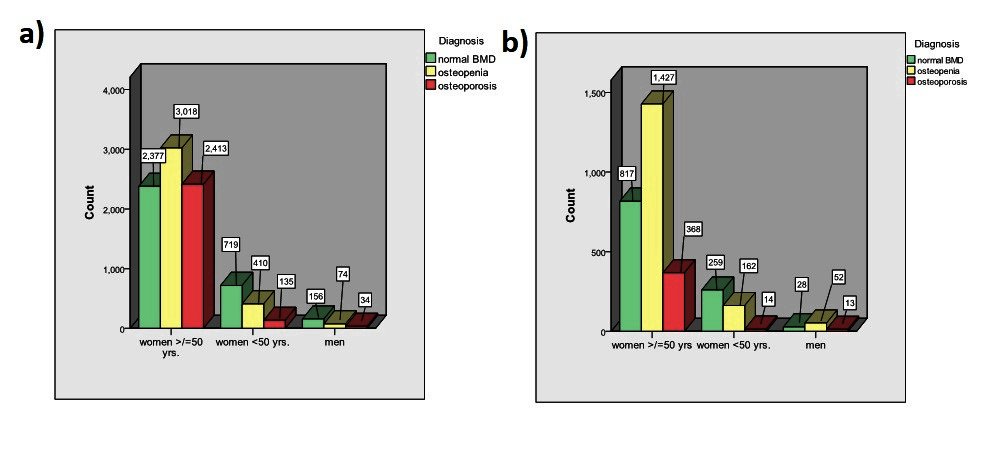
The overall prevalence of low BMD at the lumbar spine was 6 084/9 336 subjects (65.2%). 3 502/9 336 subjects (37.5%) were considered osteopenic and 2 582/9 336 subjects (27.7%) were considered osteoporotic. The prevalence of normal BMD, osteopenia and osteoporosis of the lumbar spine is shown in Fig. 2a). Osteoporosis was most frequent in the group of female subjects ≥50 yrs. with an incidence of 2 413/7 808 women (30.9%). 135 of 1 264 women (10.7%) under 50 yrs. and 34 of 264 men (12.9%) have been diagnosed with osteoporosis.

The overall prevalence of low BMD at the femoral neck was 2 036/3 140 (64.8%). 1 641/3 140 subjects (52.3%) were classified as osteopenic and 395/3 140 subjects (12.6%) were classified as osteoporotic. The prevalence of normal BMD, osteopenia, and osteoporosis of the femoral neck is displayed in Fig. 2b). Osteoporosis was most frequent in the group of female subjects ≥50 yrs. with an incidence of 368/2 612 women (14.1%). 14 of 435 women (3.2%) were under 50 yrs. and 13 of 93 men (14%) have been diagnosed with osteoporosis.
Fracture risk FRAX
FRAX MOF and FRAX HF were assessed with BMD for 1 863 subjects and the results are displayed on figure 3 in different age decades between 40 and 90 yrs. The mean FRAX MOF was 7.02%±4.14 SD (range 2-33%) and the mean FRAX HF was 1.42%±2.17 SD (range 0-20%). The mean values of FRAX MOF and FRAX HF increased significantly with increasing the age interval (p=0.000 for both fracture risk groups). 211 subjects between 40 and 49 yrs. had a mean FRAX MOF of 3.17% and mean FRAX HF of 0.31%. 667 subjects aged 50-59 yrs. had a mean FRAX MOF of 4.89% and a mean FRAX HF of 0.67%. 612 subjects in the age interval 60-69 yrs. were with mean FRAX MOF 7.73% and mean FRAX HF 1.34%. 316 subjects aged 70-79 yrs. had a mean FRAX MOF of 11.18% and a mean FRAX HF of 3.02%. 57 subjects with age 80-89 yrs. were with mean FRAX MOF of 15.38% and a mean FRAX HF of 6.13%. The median values for FRAX MOF and FRAX HF increased in the age decades whereas the age interval was 80-89 yrs. showed the highest median value for both groups.
__median__third_quartile_(q3)__max.jpeg)
DISCUSSION
This is the first study presenting large data about BMD and T-score values of the axial skeleton from DXA scans in the Bulgarian population. A previously published study in Bulgaria showed DXA scan results of the forearm for 8869 women aged 20-87 yrs. The incidence of osteopenia in this study was 28.8% and the incidence of osteoporosis was 15.16%.17 Another published study with an overall of 2 600 Bulgarian female subjects presented a 37.31% prevalence of osteoporosis at the spine and 16.14% prevalence of osteoporosis at the left hip in women aged 50 and older.18 In our study among 12 119 female subjects the incidence of osteoporosis at the spine in women aged 50 and older accounted for 30.9% which was 7% lower than those incidences presented by Boyanov et al. Largest epidemiological osteoporosis trial among 1 331 women aged 50 years or older in Bulgaria identified 16.8% incidence of osteoporosis of the femoral neck.19 The prevalence of osteoporosis at the femoral neck in women aged 50 and older in our study amounted to 14.1% which was 2.7% lower compared to the study of Borissova et al.
According to the new Scorecard for osteoporosis in Europe SCOPE 2021 the overall incidence of osteoporosis for all 27 countries of the European Union, England and Switzerland amounts to 22.1% for women and 6.6% for men. In men over the age of 50 years, the prevalence of osteoporosis varied from 5.7% (Slovakia) to 6.9% (Sweden). In women, the prevalence ranged from 19.3% (Cyprus) to 23.4% (Italy).1 In a Turkish study with 3 862 DXA measurements in female and male subjects the overall incidence of osteoporosis at the lumbar spine was 49% in Muğla and 40.8% in Erzurum which was higher compared to our overall incidence of the lumbar spine (27.7%).20 In a Greek study among 10 142 females aged 20-90 years, the prevalence rate of osteoporosis was lower (15.3%) at the lumbar spine as compared to our study (27.7%) and higher (17.7%) at the femoral neck than our study (12.6%).21 Romanian study among 622 menopausal women showed similar incidence of osteoporosis at the lumbar spine (27%) compared to our study (27.7%).22 In a Serbian study in 130 postmenopausal women the prevalence of osteoporosis was 43% at the spine and 17.7% for the total hip and these incidences were higher compared to our study (27.7% for the lumbar spine and 12.6% for femoral neck).23 Häussler et al. reported data from one health insurance fund covering 1.5 million beneficiaries in Germany and calculated that, in 2003, the frequency of osteoporosis at the femoral neck in women aged 50 years and older with osteoporosis was 39% and in men aged 50 and older was 9.7% at the femoral neck.24 In Sweden approximately 6% of the men and 21% of the women aged 50–84 years were classified as having osteoporosis at the femoral neck.25 In the United States according to the National Health and Nutrition Examination Survey (NHANES) study 2005-2006, 10% of the women and 2% of the men aged ≥50 yrs. had osteoporosis at the femoral neck.26 According to NHANES data for the period 2017–2018 the prevalence of osteoporosis at either the femoral neck or lumbar spine or both among adults aged 50 and over increased as compared to NHANES study 2005-2006 up to 19.6% for women and up to 4.4% for men.27 These incidences were lower compared to our study. The prevalence of osteoporosis in a Spanish study among 824 postmenopausal women over the age of 50 yrs. was estimated as 27.0% for the lumbar spine, which was lower compared to our study (30.9%), and 15.1% for the femoral neck, which was minimally higher than those in our study (14.1%).28
This is the first study in Bulgaria that compares BMD values between age decades in three subject groups: women under 50 yrs., women aged 50 yrs. and over and men. Interestingly, in the group of female subjects younger than 50 yrs. the lowest mean BMD value was shown at the ages below 20 yrs. Similar results were observed in the group of men where the lowest mean BMD values were presented at the ages of less than 20 yrs. for lumbar spine and in the age intervals less than 40 yrs. for femoral neck. We suggest that the reason for these results could be explained by the fact that young subjects undergo DXA scans mostly if they have some disease or use medications which could lead to osteoporosis. Above the age of 50 yrs. in the group of females, the lowest mean BMD value at the lumbar spine was presented at ages after 90 yrs. and those at the femoral neck in the age interval 80-89 yrs. The higher mean BMD value at the femoral neck in women aged 90 yrs. and over compared to the age interval 80-89 yrs. could be due to limited data available for the ages over 90 yrs. (7 subjects) or due to severe scoliosis, osteophytes, etc. which could lead to falsely elevated BMD values. After the age of 50 yrs. in the group of males the lowest mean BMD has presented in the age decade 60-69 yrs. for the lumbar spine and in the age decade 70-79 yrs. for the femoral neck.
In the current study, the mean FRAX MOF for all subjects was 7.02% and the mean FRAX HF was 1.42%. A Previous Bulgarian study reported a mean FRAX MOF of 13.4±9.2% and mean FRAX HF of 2.8±5.2% which was higher compared to our study may be due to the absence of subjects aged 40-49 yrs. and the absence of male subjects.19 Recent published studies presented that women had higher fracture probabilities than men.29 Mean FRAX MOF values differed between the European countries - 7% in Spain, 9.4% in France, 12% in Germany and Italy and 21% in Sweden.7 Spanish studies investigated only patients with osteoporosis and reported mean FRAX MOF and FRAX HF of 8.6 ± 7.35% and 3.36 ± 4.64% respectively, which was higher than our mean values.30 Palestinian studies reported lower mean fracture risk compared to our study - 3.7% for FRAX MOF and 0.3% for FRAX HF.16 These results show that fracture risk differs between the countries and the use of a specific national FRAX model is needed.
Limitations
The studied sample consisted of patients which were selected by physicians to conduct DEXA scan and was therefore not random. Furthermore, the UK FRAX algorithm was used to calculate FRAX MOF and FRAX HF due to the absence of a national model for the time period 2011 to 2019.
CONCLUSION
This study is the largest epidemiological research in Bulgaria up to date about the prevalence of low BMD using DXA scans at axial sites for 12 478 subjects. The overall prevalence of low BMD at the lumbar spine was 65.2% and at the femoral neck, the prevalence was 64.8%. The overall incidence of osteoporosis at the lumbar spine was 27.7% and at the femoral neck was 12.6%, which was lower than the values reported in previous published Bulgarian studies.
Acknowledgments
None
Author contributions
Elena Kirilova, Nikola Kirilov, Stoyanka Vladeva, Nikolay Nikolov, Martin Nikolov, Anastas Batalov, Zguro Batalov, Plamen Kinov, Vihar Kovachev, Mancho Kovachev and Svilen Todorov contributed equally.
Conflict-of-interest statement
The authors declare that they have no competing interests.
Supportive foundations
None