Introduction
Over 80% of people will experience one or more episodes of low back pain at some point in their lives with many of these episodes self-resolving within 4-6 weeks.1–4 Often, the acute episode of low back pain will become chronic, lasting greater than 12 weeks.5 The resulting economic burden, whether it be acute or chronic low back pain, can be quite substantial with estimates reaching well over $100 billion dollars annually not including the lost wages due to lack of productivity.6,7 As the population ages, so will the overall number of sufferers of chronic low back pain and the costs associated.
The initial treatment of low back pain is conservative pharmacologic and nonpharmacologic management including, but not limited to, nonsteroid anti-inflammatory agents and physical therapy.8,9 When patients fail conservative management, the decision to pursue imaging to identify a source is then undertaken. Depending on the cause of the low back pain, minimally to more invasive techniques are used to target the source of low back pain. When surgical interventions such as back surgery fail to treat the source of pain, other options can be used to treat the resulting persistent pain after spinal surgery.
Spinal cord stimulator (SCS) is a Federal Drug Administration-approved treatment modality for treating persistent pain after spinal surgery, complex regional pain syndrome, and painful diabetic neuropathy.10,11 Patients first undergo a SCS trial by placing electrodes in the epidural space with a temporary external power source to determine if the patient achieves relief.10 The pulses generated by traditional SCS may create paresthesias that overlap in the region of pain. If the trial is successful, a permanent SCS is implanted. However, the use of paresthesias in low frequency SCS may be uncomfortable or undesired by many patients.10 To avoid the use of paresthesias, a 10kHz waveform at a sub-perception threshold can be used to provide superior pain relief without the sensations provided by traditional SCS [Nevro Corp., Redwood, CA, USA].12,13
Here we describe our experience utilizing 10kHz therapy to salvage a failing SCS trial. The patient ultimately achieved superior pain relief with 10kHz therapy.
Case Description
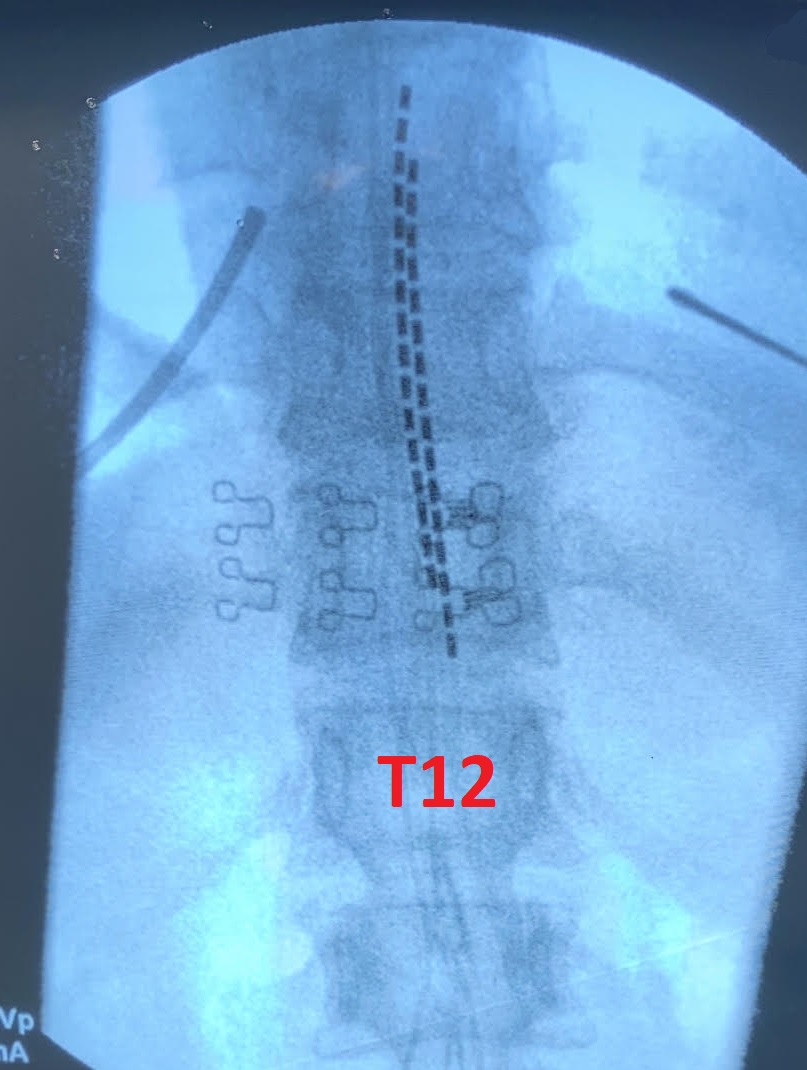
The patient was a 66-year-old female who underwent a laminectomy and fusion at L4/5 several years prior for persistent back pain complaints not responsive to more conservative options. She presented to the pain clinic after undergoing physical therapy for 6 months with no benefit along with multiple failed epidural steroid injections as well as radiofrequency ablation procedures without significant improvement in her pain complaints. She was being managed with intermittent trigger point injections along with pharmacological treatments including acetaminophen, NSAIDs, membrane stabilizers, muscle relaxers and opioids. The patient underwent psychological testing and was deemed a good candidate for SCS trial for her chronic debilitating back pain complaints. She underwent a SCS trial placing two 16-contact leads at the top of the T7 vertebral body and paresthesia mapping for pain coverage. The patient reported dissatisfaction with her pain relief 4 days into her trial. A fluoroscopy image was obtained demonstrating no lead migration. The leads were pulled down so that the top 8 contacts covered the T9/10 disc space and the patient’s SCS leads were switched to over to Nevro and 10kHz stimulation. (Figure 1) The patient reported gradual improvement in her pain complaints and after another 4-day trial period she reported greater than 70% improvement in her pain complaints and improvement in her quality of sleep. She proceeded to permanent implantation with similar results.

Discussion
Chronic low back pain continues to affect the lives of hundreds of millions worldwide.1,7 When conservative management fails, interventional options should be considered in these patients. When traditional intervention pain management procedures have been exhausted or the patient has persistent back pain after spine surgery, SCS should be explored as a potential option for providing pain relief. SCS therapy is minimally invasive and reversible. It can be used to treat a wide variety of neuropathic pain syndromes.11–19 Additionally, there is also growing evidence supporting the use of 10kHz SCS for patients with chronic back pain who are not interested in structural surgery or deemed not a surgical candidate.13,20
When traditional SCS proves ineffective, switching to 10kHz stimulation should be considered. Compared to low frequency SCS, 10kHz stimulation can provide superior pain relief that is sustained along with reduction in opioid consumption. 12,21,22 Our case demonstrates the ability to switch therapies during the middle of a SCS trial to another company to provide a different therapy. There are a few key points that should be highlighted when considering this option:
-
Consider re-imaging initial trial SCS leads to ensure inadequate coverage is not due to lead migration.
-
Consider the initial lead placement as traditional SCS leads are commonly placed higher or in different locations due to parasthesia mapping. 10kHz leads are commonly placed anatomically at the top of T8 and T9 to cover the T9/10 disc space.
-
We recommend utilizing proper sterile and clean techniques when repositioning the leads. We typically reclean the area with chlorhexidine and utilize sterile gloves to reposition the leads.
-
Reposition the leads under fluoroscopy to the desired location.
-
We do not recommend advancing the leads if they have migrated down out of position, we only recommend withdrawing the leads down over to the desired location.
-
When the previous system does not utilize 8 contacts per lead, consult with your Nevro representative regarding which contacts can be utilized. In our case they could only utilize the top 8 contacts, so these were pulled down to cover the T9/10 disc space.
Conclusion
In patients with chronic debilitating neuropathic pain that is not responsive to traditional SCS therapy, transitioning these patients to 10kHz therapy may prove to be a valuable option which can lead to significant improvement in pain complaints and salvage a failing SCS trail. This case demonstrates the ability to transition a patient to 10kHz in the middle of a trial and highlights important concepts to consider when transitioning a patient to a different therapy in the middle of a SCS trial.