


1. INTRODUCTION
Spontaneous osteonecrosis of the knee (SONK) was described first in 1968 by Ahlbäck et al.1 SONK can be classified in primary and secondary osteonecrosis. While the former has idiopathic etiology, the latter can be due to factors such as steroid therapy, systemic lupus erythematosus, alcoholism and hemoglobinopathies. Evidences suggest that chronic stress, insufficient blood supply, or minor trauma may result in a weakened subchondral bone, which could present as subchondral insufficiency fracture or focal subchondral osteonecrosis.2 The disease typically affects patients fifty to sixty years or older. Female patients are affected three times more often than men. The classic patient is active, and with a history of osteoporosis or osteopenia.3 The onset of symptoms is usually rapid without trauma or strain. Patients complain pain on the affected side especially with load and less in rest. The X-rays are in the beginning often normal or might show a radiolucent lesion in the subchondral area. Findings in X-rays can be elucidated by magnetic resonance imaging (MRI). MRI is especially useful in the early stages of the disease, with its high sensitivity to detect bone edema. MRI findings usually include bone marrow edema localized to the medial femoral condyle, which may spread to the intercondylar notch. Additionally, a subchondral crescent of a linear focus of low signal intensity can be seen on the T1-weighted sequences.4 Concurrent meniscal tears are also common and can be diagnosed accurately on MRI as well. SONK is a progressive disease. Conservative treatment is recommended in the early stage of the disease for small lesions without evidence of structural ruin. For lesion width > 50% of the condyle, the conservative treatment shows poor results. The advanced stages are generally treated with surgery such as: drilling, osteochondral grafts, high tibial osteotomy with or without bone grafts, or unicompartmental knee arthroplasty (UKA) and total knee arthroplasty (TKA). Soucacos et al.5 suggested surgery for SONK stage III or higher. SONK is usually localized and circumscribed in the medial compartment of the knee; therefore, unicompartmental knee arthroplasty (UKA) appears to be a tailored treatment option. Different studies suggest its utility in the treatment of osteonecrosis of the knee. Unfortunately, due to the relative rarity of SONK, these studies often lack patient numbers and control groups, and have short follow-up, thus making it difficult to draw conclusions. To address these limitations, we plan a systematic review to evaluate all available current literature on UKA in the setting of SONK. The aims of this systematic review are to determine the clinical and functional outcomes and understand the survivorship in patients who undergo UKA in the setting of SONK.
2. MATERIALS AND METHODS
2.1. Literature search
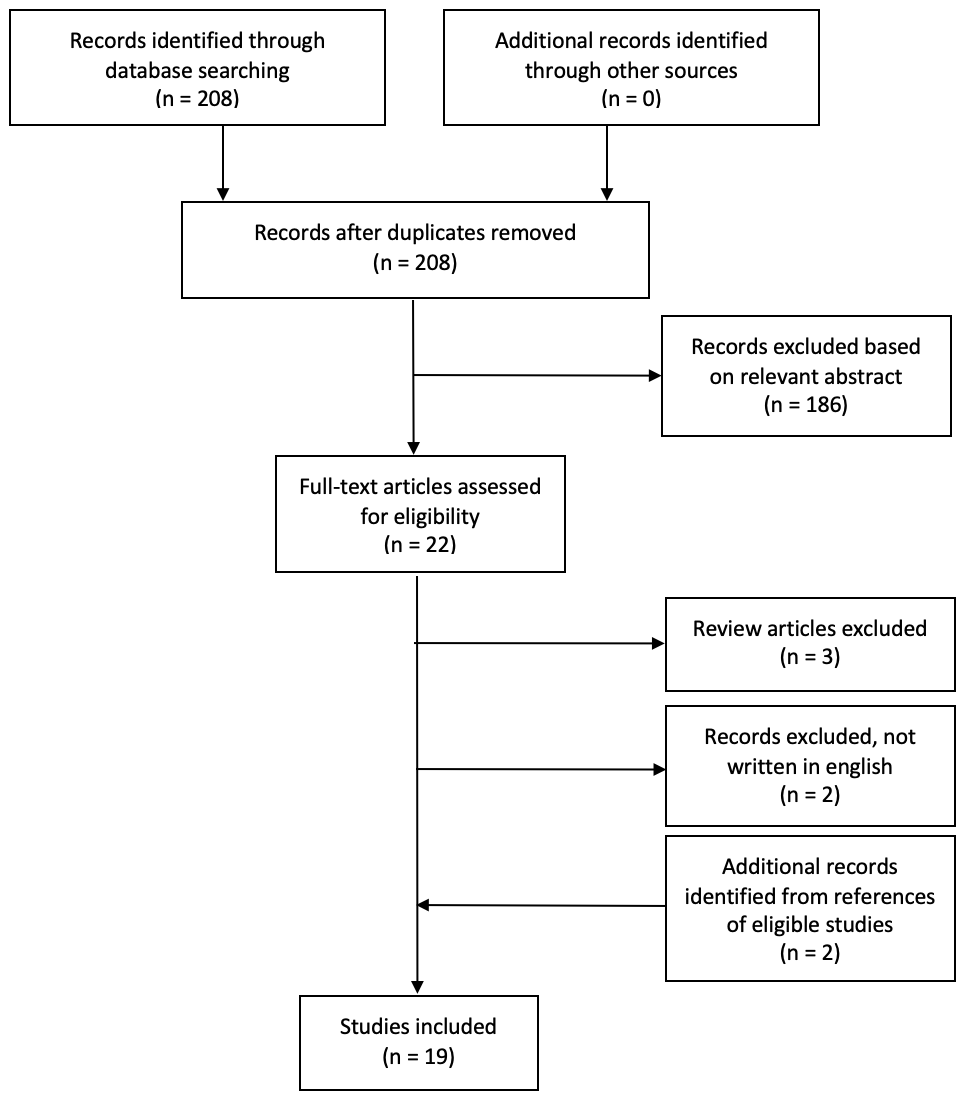
A systematic review of the literature was performed according to the “Preferred Reporting Items for Systematic Reviews and Meta-Analyses” (PRISMA) guidelines with a PRISMA checklist and algorithm.6 The search algorithm according to the PRISMA guidelines is shown in Figure 1.
_research_flo.png)
A comprehensive electronic search was performed using the PubMed, Embase, Web of Science, and Cochrane databases to evaluate all studies examining patients who underwent UKA for SONK. The search string for title and abstract screening consisted of different combinations of keywords:
“unicompartmental AND osteonecrosis” (131 studies) and “UKA AND osteonecrosis” (77 studies). The search was performed in November 2021. Two authors (L.S. and P.Z.), independently blinded from each other’s results, further examined the title and abstract of these studies, finding that 40 were relevant.
2.2. Inclusion/exclusion criteria
Studies were selected with predetermined inclusion criteria: 1) studies that specifically assessed SONK treated with UKA; 2) studies reporting implant survival rate and global clinical outcomes; 3) studies with a minimum follow up of 1 year. Exclusion criteria were: articles not written in English, articles that did not differentiate between primary and secondary osteonecrosis of the knee in their results, articles published before 2000. Literature reviews, studies on cadaver or in vitro investigations, biomechanical reports, technical notes, letters to editors were also excluded. We also reviewed the references for each of the included papers to identify other potential studies that were missed. The senior authors (E.F. and S.C.) intervened to reach a final decision if the reviewers disagreed about the inclusion of a study.
2.3. Full text screening and extraction of data
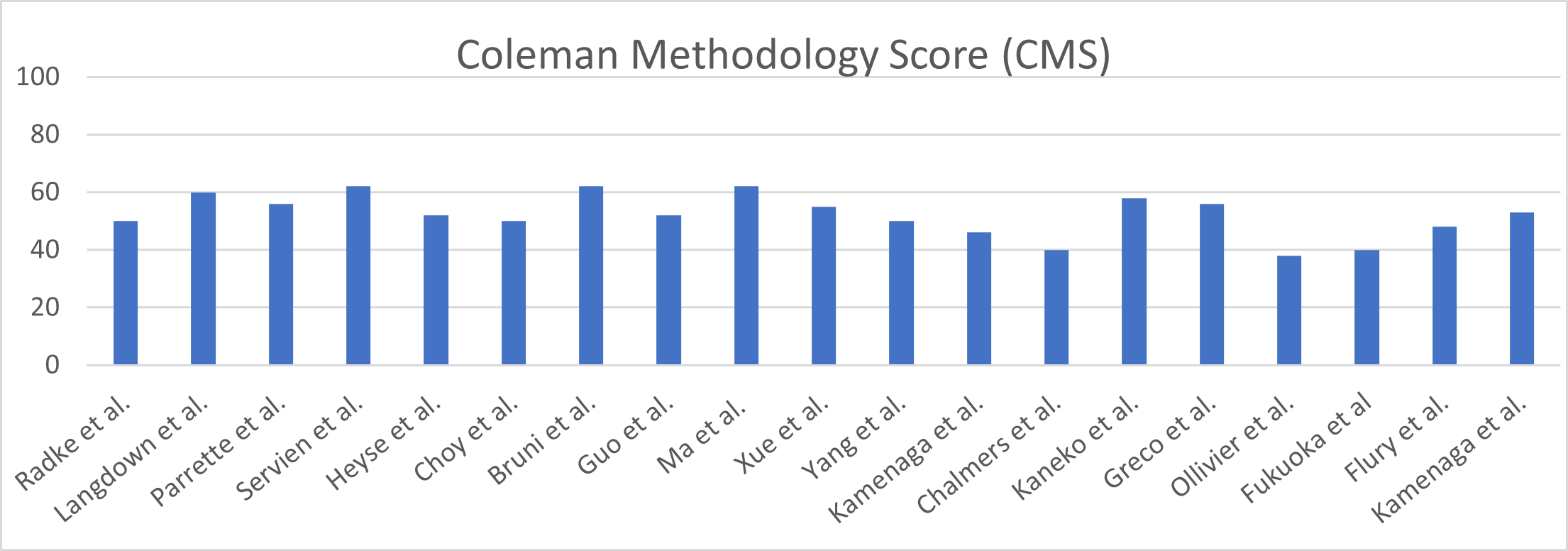
After title and abstract screening, a full-text analysis was performed in which articles were excluded if the required inclusion criteria were not met. Extracted data included years of follow-up, patient demographics (age, gender, BMI), laterality of lesion, unicompartimental knee arthroplasty implants, reason for revision (aseptic loosening, superficial and deep infection, and poly wear…), revision rate, maximum knee flexion and knee clinical outcomes score and Kaplan-Meier survival curves. All data were compiled in a Microsoft Excel spreadsheet (2021v; Microsoft Corporation, Redmond, Washington, USA). The categorical variable was reported as frequency with percentage. Continuous variable data were reported as mean value with the range between minimum and maximum values. In all studies, P < .5 was considered statistically significant. The level of evidence (LOE) of the included studies was assessed according to the “The Journal of Bone and Joint Surgery” criteria.7 To assess the quality of the studies, the Coleman Methodology Score (CMS)8 was used, which assesses methodology with 10 criteria, giving a total score between 0 and 100 (Table 1). A score of 100 indicates that the study largely avoids chance, various biases, and confounding factors. Each study was scored by two reviewers (L.S. and P.Z.), independently. Then, disagreements were resolved by discussion with other two reviewers (E.F. and S.C.) and final scores were assessed and wrote down (Figure 2).
.jpg)
.png)
3. RESULTS
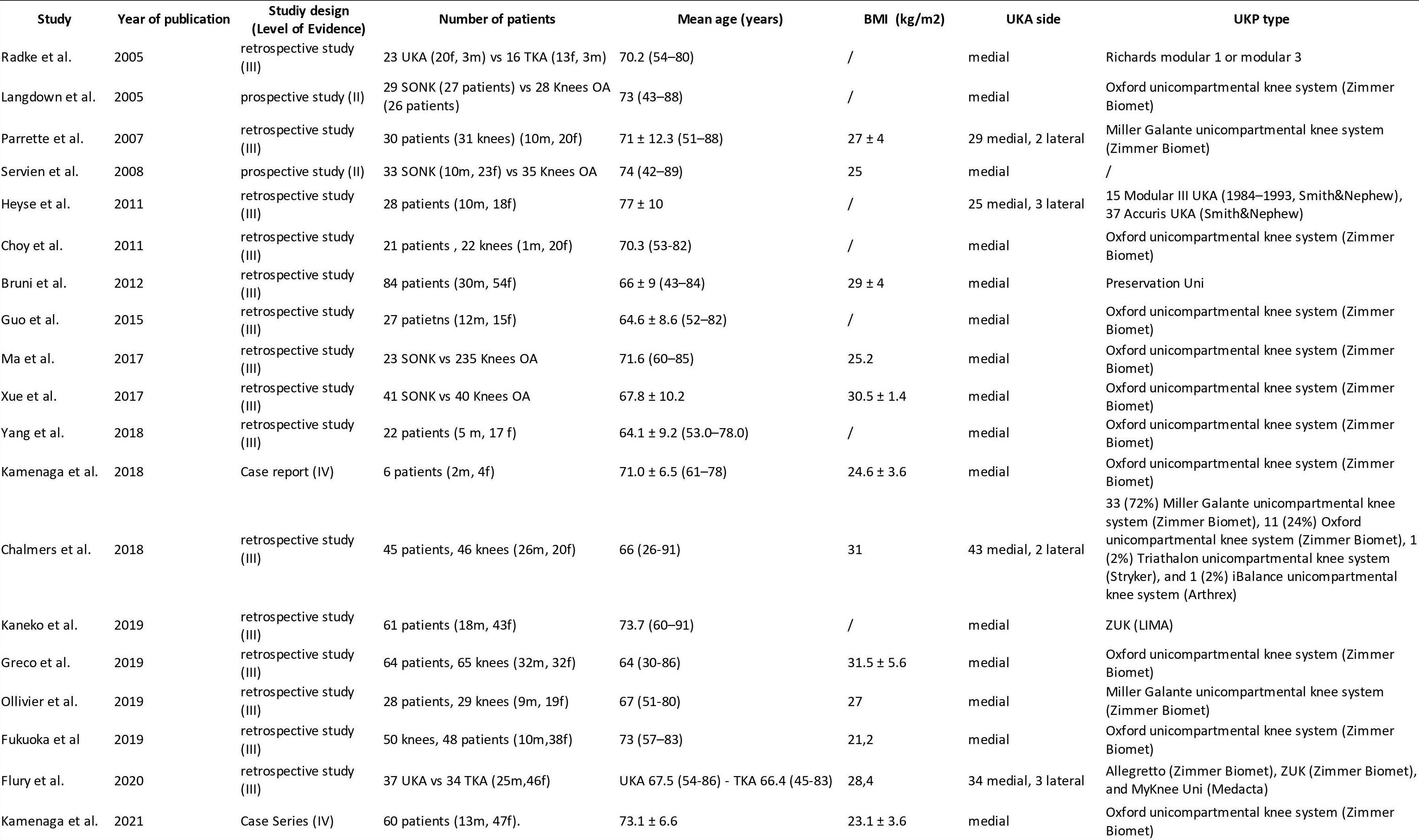
In total, 208 articles were identified using the search string. Only 143 articles then fulfilled the inclusion criteria and thus proceeded to full-text analysis. After examination of the full texts, two records were identified from the reference of included articles, and 19 studies9–27 were finally included in the systematic review, as summarized in the PRISMA flow chart (Figure 1): 2 prospective studies, 1 case report, 1 case series with the remaining 15 retrospective studies. We extrapolated the data of a total of 717 unicompartimental knee arthroplasty procedures to treat osteonecrosis of the knee. 693 patients (96,65%) had SONK while only 24 patients (3,35%) were affected of secondary osteonecrosis of the knee, mainly due to steroid therapy. It was not possible to exclude this small part of outcomes from the others. All patients’ demographics data are resumed in table 2. These patients had a mean age of 68 years (range 64-74 years). There was a 2:1 ratio of female to male (436:206, from 642 patients (89,53%) of 16 studies), with a mean body mass index (BMI) of 26,5 kg/m2 (range of means 23,1-31,5 kg/m2 from 499 patients (69,59%) of 12 studies). There was only 10 lateral UKA (1,39%), with the remaining medial UKA (98,61%). In the 19 studies included in our review, the patients were treated with several types of unicompartimental knee arthroplasty implants, in particular: Oxford unicompartmental knee system (Zimmer Biomet), Allegretto (Zimmer Biomet), ZUK (LIMA), and MyKnee Uni (Medacta), Triathalon unicompartmental knee system (Stryker), iBalance unicompartmental knee system (Arthrex), Modular I-III UKA (Smith&Nephew), 37 Accuris UKA (Smith&Nephew), Miller Galante unicompartmental knee system (Zimmer Biomet) and Preservation Uni.

3.1. Clinical Outcomes
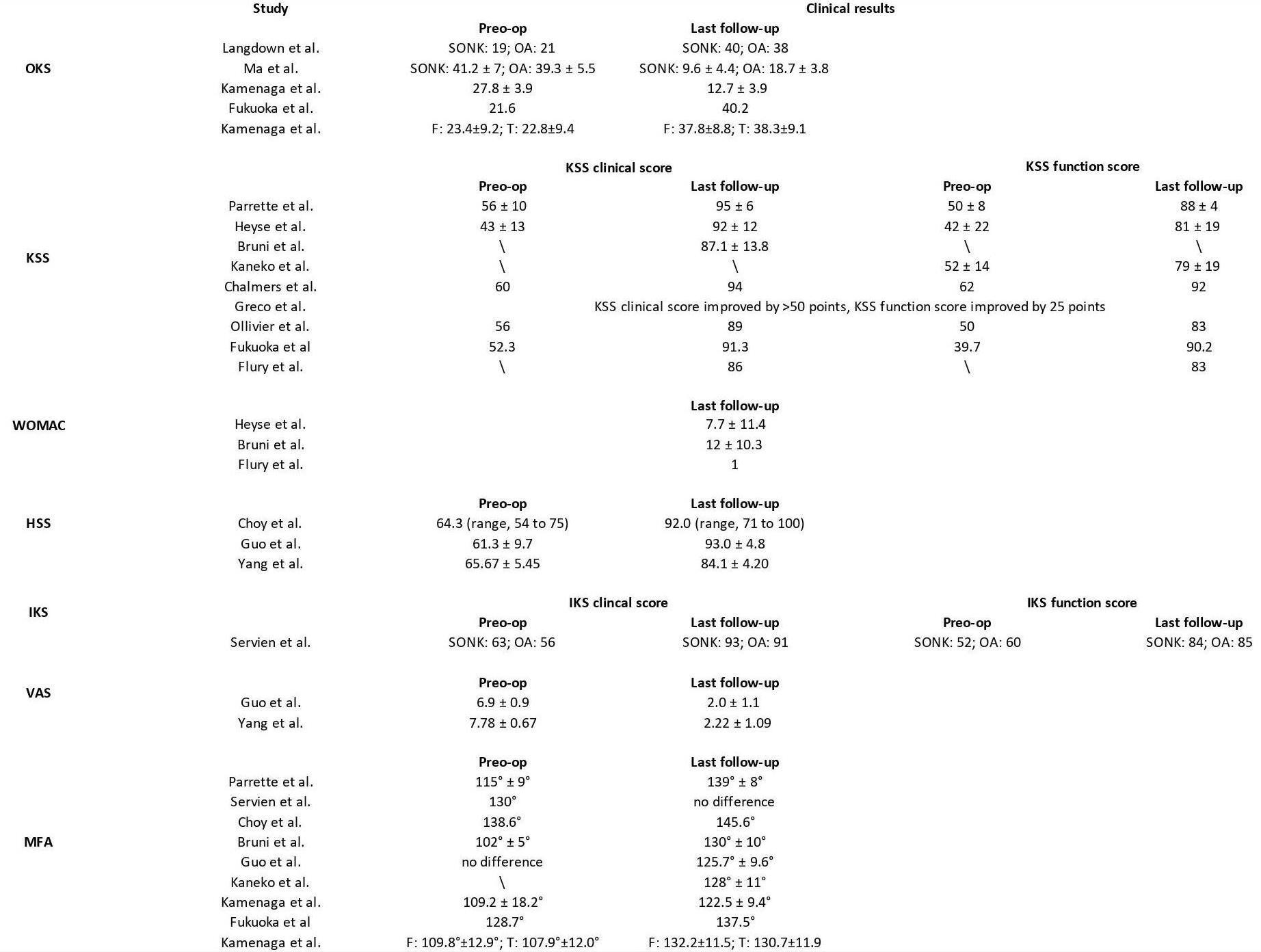
In the 19 studies included in our review, we find several types of clinical scoring systems, in particular: Oxford Knee Score (OKS) in five studies,14,15,17,18,27 Knee Society Score (KSS) in nine studies,12,13,16,19,21,22,24,25,27 Western Ontario and McMaster Score (WOMAC) in three studies,19,22,25 Hospital for Special Surgery knee score (HSS) in three studies,9,20,23 International Knee Score (IKS) in one study.10 In addition, Visual Analogue Scale (VAS) for pain were reported in two studies9,20 and the Mean Flexion Angle (MFA) were reported in nine studies.10,12,17,18,20,23,25,27 All patients’ clinical outcomes are resumed in table 3. The data collected note that UKA in the setting of SONK had acceptable to good clinical outcomes both in the short- and long-term.
3.2. Radiological findings, failures and survival rate
The mean follow-up, radiological findings about radiolucency lines (RLL), failures details and survival rate of each studies included are resumed in table 4. Interestingly, only 12 cases of aseptic loosening out of a total of 717 surgical procedures performed were described until the last follow-up, and only 8 cases of periprosthetic fracture.

3.3. Methodological Evaluation
The Coleman Methodology Score (CMS) (Table 1)8 was used to assess the quality of the design of the studies included in the present systematic review (Figure 2). The average value was 52.1, ranging from 3813 to 62.14,25 Therefore, the overall level of methodological quality of the included studies was low.
4. DISCUSSION
UKA is considered a less aggressive surgery than TKA, thanks to the ligament preservation and reduced bone resection. As compared with TKA, UKA has been shown to have a shorter operative time with less blood loss, shorter hospital stays, earlier rehabilitation, improved gait kinematics and better ROM, earlier return to sports28; furthermore it has been reported high forgotten joint score29 and good survival outcomes,30 but the rate of revision in national registries is three times higher.31–33 Caution is needed when performing UKA in patients with SONK primarily due to doubt bone quality of SONK lesion and surrounding area that may affect the implant fixation. Therefore, further evaluation is needed to determine the clinical and functional outcomes and the survivorship in patients who undergo UKA in the setting of SONK. We compared the clinical outcomes and survival rate of UKA in SONK using the results of previous 19 original studies9–26 (Table 1) and the collected data show how UKA can be an acceptable procedure for the treatment of primary SONK, when it is correctly indicated in a carefully selected patients. Radke et al.11 retrospectively evaluated 23 UKAs and 16 TKAs after a mean follow-up of 5 years. This study shows worse clinical long-term outcomes and a higher revision rate in patients undergoing UKA, which they attributed mainly to secondary progression of osteoarthritis in the uninvolved compartments. However, their results are limited to the small case series and lack of contemporary implant designs (UKA arthroplasty Richards modular 1 or modular 3, Tuttlingen, Germany), with all UKAs implanted before 1988. Moreover, the risk of overall revision was similar in both cases. In a much more present study, Flury et al.22 compare the outcomes of a larger cohort of 71 patients affected of SONK treated with either UKA or TKA. With a mean follow-up of 6.6 years, UKA showed slightly superior functional outcomes. The two treatment groups showed no significant difference in all radiographic parameters took in consideration. The overall complication rate was higher when compared to TKA (2 failures in TKA group vs 4 failures in UKA group, RR 1.83), but it was not significance (p = 0.4). Bruni et al.25 retrospectively studied the survivorship of medial UKA performed for late-stage spontaneous osteonecrosis of the knee in 84 patients with medial compartment SONK, with a mean follow-up of 10 years. The overall survivorship was 89%, the most common causes of revision were related to complications affecting the tibial component, although only 7 patients examined had medial tibial hemi-plate SONK. The authors do not specify whether osteonecrosis of the tibial plateau may have adversely affected the revision rate. In this regard, in a recent case series of 60 patients, Kamenaga et al.17 observe short-term and midterm outcomes following UKA to determine whether tibial lesion affects the procedure clinical and radiographic outcomes. Patients diagnosed with SONK in the medial femoral condyle and treated with UKA were separated into two groups using MRI: group F (necrotic lesion confined to the femur) and group T (necrotic lesion spread to the tibia). Results from this paper argue that osteonecrosis of the tibial plateau does not affect clinical and radiographic outcomes in the short and midterm. These data are confirmed by the results from some national registries: a recent review of 5351 UKAs from the Norwegian registry found survivorship of 81% at 10 years follow up; similar registry studies from New Zealand and Sweden have reported ten-year survival rates of 89% and 86%, respectively.32 Servien et al.10 report a prospective series of 33 UKA operated for SONK compared with 35 UKA operated for OA. At the last follow-up, the survival rate was 92.8% for the SONK group and 95.4% for the OA group, with comparable outcomes in terms of pain, knee score and function. About radiological findings, they found a higher number of radiolucent lines in the SONK group. These lines were most frequently on the tibial side but were considered stable, no evolutional in all cases and none of these patients underwent reoperation. Parratte et al.12 found a survival rate of 96.7% at 12 years, although only 30 patients (31 knees) were included in their retrospective study and no information is provided regarding the size of the femoral or tibial lesions. Greco et al.21 characterized the size of the osteonecrosis in 64 patients (65 knees) but did not find a correlation between lesion size and quality of implant fixation. However, the follow up is limited to 5.3 years and the case series is poor. This result was confirmed by Fukuoka et al.27 with a follow up of 15 years. Despite these promising results, it is essential to underline how a correct surgical indication and correct patient selection are essential to obtain an optimal result. Canonical indications widely used for unicompartimental knee replacement should be carefully observed, reserving the procedure to knees with strictly unicompartmental joint disease. Furthermore, a careful distinction between spontaneous and secondary osteonecrosis should be made during the diagnostic process, given that some studies have reported worse results in case of usage UKA in secondary osteonecrosis by the propensity for subsequent multicompartment involvement.24,25 Presence of an idiopathic necrotic focus does not seem to influence the revision rate, specifically this does not seem to cause increasing of aseptic loosening complications. In fact, most of the reviews carried out were not associated with causes directly attributable to osteonecrosis, but mainly to the progress of osteoarthrosis in the contralateral compartment or to infections or complications affecting the tibial component; it should be noted that UKA’s revision rate is related to the number that surgeons implant, with those who are small in number having high revision rates.31 Although our study does not focus on alternative procedures to UKA and TKA for the treatment of SONK, several other procedures have been reported in the literature with varying success. These include arthroscopic debridement, microfracture, core decompression, and osteochondral allograft transfer system procedures; however, these procedures are not recommended for the treatment of advanced osteonecrosis due to prolonged morbidity.
4.1. Limitations
This study has limitations typical of a systematic review. These limitations included the fact that we may have missed some pertaining articles. This chance was minimized with two separate investigators who conducted individual literature searches and cross-referenced each paper to ensure completeness. The small number of low-evidence studies with a prevalent retrospective design is a relevant limitation. Most of the papers are limited by small sample sizes and a relatively short follow-up period. Furthermore, the heterogeneity of the outcome measures, the differences in follow-up periods, and the design of the prosthesis did not allow grouping the results nor a quantitative analysis. We were careful to list each data from each paper separately in the project’s electronic spreadsheet to ensure accurate measurements and proper units for correctness. There is also a risk that our data could be partially misunderstood due to the scaled adjustment for clinical scores. However, this was necessary to obtain more meaningful results from the collected data.
5. CONCLUSION
With the present systematic review of the literature, we advocate that UKA can be an acceptable procedure for the treatment of primary SONK when it is correctly indicated in a carefully selected subset of patients. UKA had acceptable survival analysis as well as revision rates and good clinical outcomes both in the short- and long-term. We would encourage to establish a unique radiological classification that can be used uniformly and make the various studies easily comparable. Furthermore, the current classifications do not allow to make a clear correlation between radiological stage, recommended treatment, and prognosis. As it is clear, the reported results of UKA for osteonecrosis of the knee are relatively few and are limited to mostly retrospective case reports and cohort series with small patient numbers and short or mid-term follow up. It is necessary to promote further studies to investigate the issues that are still not documented in an exhaustive and irrefutable way. Prospective, randomized, double- blind studies, on a large sample of the population and with a longer follow-up, would give us fundamental answers for the correct understanding of the advantages, but also of the limits and contraindications, in the use of UKA as a definitive treatment for localized SONK.
Author Contributions
Conceptualization L.S.; methodology, L.S. and P.Z.; validation, E.F. and S.C.; investigation, L.S. and P.Z.; data curation L.S., P.Z. and G.F.P.; writing original draft, L.S., P.Z. and C.E.; writing review and editing, E.F, S.C. and B.Z.; supervision and project administration, N.P. and R.P.
All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.