INTRODUCTION
Approximately 200,000 anterior cruciate ligament (ACL) injuries occur each year in the United States, and approximately 40-60% of cases are associated with meniscal tears.1,2 Most meniscal tears are treated using partial meniscectomies or meniscal sutures, with an increasing trend towards meniscal repairs to preserve meniscal function.3,4 After lateral meniscectomies, the progression to cartilage wear, and consequently osteoarthritis, is more rapid, while medial meniscectomies have been shown to predictably cause degenerative changes in the knee.5 When an ACL tear is added, the effects of this degenerative progression are even more rapid. ACL reconstruction (ACLR) surgery results in pain relief, improved stability and increased activity level.6 However, long-term outcomes after ACL reconstruction in a knee with partial or total meniscectomy are usually worse than in a knee with intact menisci.7 Therefore, the meniscal suture is the treatment of choice for meniscal tears, and if the meniscus is not repairable, arthroscopic partial meniscectomy of the torn portions of the meniscus is recommended. Unfortunately, in some meniscal tears, the damage is so extensive that subtotal or complete meniscectomy is required, leading to a predictable pattern of progressive articular cartilage deterioration and radiographic narrowing of the joint space.8 In such cases, an alternative treatment is meniscal allograft transplantation (MAT), which is effective for post-meniscectomy syndrome and aims to restore the functional status of the meniscus by providing protection and stability to the joint.9–11 The success of the MAT procedure depends on proper indication in young patients younger than 50 years with long-standing pain, refractory to conservative therapy after a complete meniscectomy.12,13 Recently, several publications have analyzed ACL reconstruction in association with MAT, showing good clinical outcomes, overlapping with those of ACL reconstruction and MAT performed alone.14 Furthermore, while the association between the rate of return to sport (RTS) has been studied in both isolated ACL procedures and those associated with osteotomies, the return to sports activity after MAT combined with the ACLR procedure has never been analyzed.15,16
OBJECTIVES
The purpose of this study was to review the available literature regarding Meniscal Allograft Transplantation (MAT) combined with Anterior Cruciate Ligament Reconstruction (ACLR). The primary objective was to evaluate clinical outcomes. The secondary objectives were to report the complication, reoperation and RTS rates. It was hypothesized that combined treatment would ensure favorable functional outcomes and low failure rates.
METHODS
Search Strategy and Design
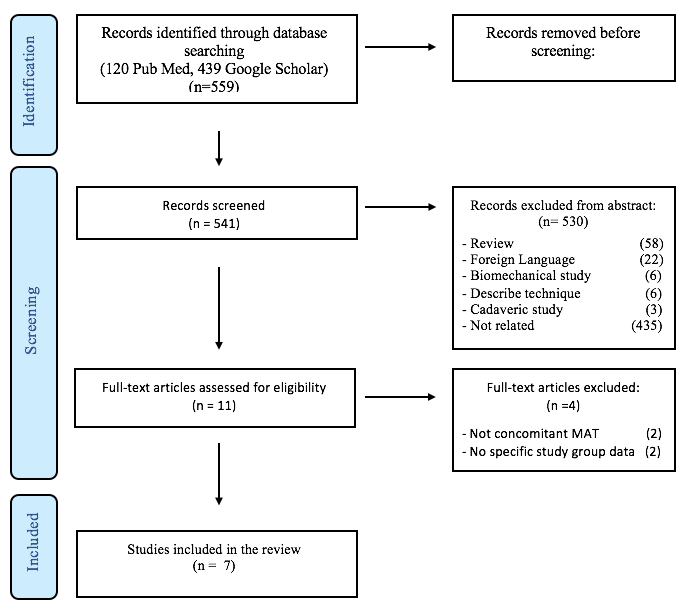
The present study was a systematic review of the literature conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. The search was performed through the following online databases: Google Scholar and Medline via PubMed. The main keywords were as follows: “Meniscal Allograft Transplantation” AND “Anterior Cruciate Ligament” and their Medical Subject Headings (MeSH) terms in any possible combination. The research was conducted without publication date limits, until December 2022 (Figure 1).

Eligibility Criteria
Inclusion criteria were: (1) cases of MAT in combination with primary or revision ACLR; (2) all levels of evidence; (3) patients of any age and gender; (4) studies published as full-text articles in indexed journals in English; (5) human studies. Exclusion criteria were: (1) manuscript without specific study group (MAT + ACLR) data; (2) surgical technical reports; (3) expert opinions or letters to the editor; (4) surveys; (5) reviews; (6) cadaveric or animal studies.
Study Selection
The selection of eligible publications was made independently by two authors (C.F. and B.V.). Articles were reviewed based on title and abstract. After the exclusion of the ineligible articles, the full texts of the remaining were reviewed. Any discrepancies were resolved by consensus of the senior author (C.S.). Finally, the reference lists of included articles were analyzed to identify further relevant studies to include in the systematic review.
Methodological Quality Assessment
The Methodological Index for Non-Randomized Studies (MINORS) checklist was used to evaluate the quality of all included studies. The maximum score was 16 for non-comparative studies and 24 for comparative studies. Each study included was scored independently by 2 authors (C.G. and C.D.).
Data Extraction and Analysis
The authors used a standardized data extraction form that included the following: (1) study details (author, year, nationality, study design, level of evidence and MINORS score); (2) study population (cohort size of case series, gender, age at the time of surgery); (3) timing information (previous meniscectomy to MAT surgery interval, mean follow-up, patients lost to follow-up); (4) surgery information (MAT surgical technique, MAT side, primary or revision ACLR setting, type of graft used for ACLR, concomitant chondral pathologies, other concomitant procedures); (5) pre- and postoperative clinical evaluation (Tegner activity scale, Lysholm knee score, International Knee Documentation Committee Scale (IKDC) score); (6) return to sport rate; (7) postoperative complications and re-operation rate.
Statistical Analysis
The kappa (k) value was used to assess the consensus between reviewers in the selection of articles and methodological quality assessment. The agreement was classified as poor with k < 0.30, partial with 0.30 < k < 0.60 and total with k > 0.60. A meta-analysis was not performed, due to the high heterogeneity between studies.
RESULTS
Literature Search and Study Characteristics
The initial search included 559 studies (120 from PubMed and 439 from Google Scholar). After excluding the duplicates, the articles were included based on title and abstract. The full texts of the remaining 11 articles were examined according to the inclusion and exclusion criteria. Finally, seven articles met the inclusion criteria of the systematic review5,14,17–21 (Figure 1).
There was a high level of agreement among reviewers regarding the title (k = 0.93; 95% CI, 0.92-0.94), abstract (k = 0.91; 95% CI, 0.89- 0.93), full text (k = 0.93; 95% CI, 0.92-0.94), and MINORS scores (k = 0.90; 95% CI, 0.88-0.92). The selected articles were published between 2003 and 2019. Five studies were retrospective case series, one of which was a comparative study. While the other two were a prospective case series and a case report.
Regarding the level of evidence, two studies had level III and five had level-IV evidence. The mean MINORS score was 11 (range 10-12) and 20, for the non-comparative studies and comparative study, respectively. The studies were conducted in the United States (57.1%), France, Germany and Italy (14.3% each) (Table 1).
Demographic Data
The initial cohort included 154 patients, of whom 25 (13.5%) were lost to the follow-up. Therefore; 133 patients (69.2% males and 30.8% females) and 138 meniscal allograft transplantations combined with anterior cruciate ligament reconstructions were evaluated. The mean age at the time of the surgery was of 35.3 years (range 19-48). The mean previous meniscectomy to meniscal allograft transplantation interval was 114.3 months (range 3-312). The mean follow-up duration was 5.3 years (range 1.1-12). (Table 1)
Surgical procedure data
Overall, 138 meniscal allograft transplantations combined with anterior cruciate ligament reconstructions were evaluated. In most cases, MAT was used to replace the medial meniscus (82.6%), while in 17.4% it was used for the lateral compartment. Different MAT techniques were used: Bone bridge technique (39.1%), MAT without bone plugs (37%) or double bone plug technique (23.9%). The MAT was associated with a primary ACL reconstruction in a primary setting in 52.6% and a revision setting in 47.4% of the cases. The most common graft was bone patellar tendon bone (BPTB) (57.5%), followed by Achilles tendon (31%), Tibialis anterior (4.6%) and Hamstring (3.4%). Concomitant chondral pathology was assessed with different classifications: Noyes grading system, Outerbridge classification and the International Cartilage Repair Society classification. (Table 2).
Functional outcomes and rate of return to sport
The mean pre- and postoperative values of the Tegner activity scale, Lysholm knee score and IKDC score are shown in Table 3. The mean improvements were 1.8, 26.7 and 24.7 on the Tegner activity scale, Lysholm knee score and IKDC score, respectively. Regarding sports activities, it was not reported in 9 patients (2 manuscripts), while 102 played sports before symptoms. 77 (75.5%) returned to sports practice after the MAT + ACL procedure. In all studies reporting sports practice information, the level of RTS was lower than that before the onset of the symptoms. (Table 3)
Complications and Re-operation Rate
No intra-operative complications were reported. The overall postoperative complication rate was 11.6%. Minor complications (superficial infections) were reported in 2 cases (1.5%) and major complications (MAT or ACL failures) were reported in 14 cases (10.1%). A total of 33 re-operations were documented (23.9%), including 6 (4.3%) cases of total knee replacements (Table 4).
DISCUSSION
The most important finding of the present review is that postoperative clinical and functional outcomes show significant improvement over preoperative outcomes (Tegner activity scale, Lysholm knee score and IKDC), after ACLR associated with MAT. In addition, a high rate of return to sport (77.5%) and a moderate rate of postoperative complications (11.6%) were observed. MAT is a valid treatment in patients with a previous total or subtotal meniscectomy. Some authors have highlighted the biomechanical benefit of MAT in patients with a previous ACLR. Spang et al,22 in a cadaveric study, showed that MAT reduces the strain on the native ACL, thus providing evidence supporting the use of MAT in ACL-reconstructed knees. However, combined MAT+ ACLR is an uncommon and challenging procedure which should be performed by highly trained knee surgeons. The indications for this procedure are limited to young patients with knee instability secondary to an ACL injury or failed ACL reconstruction associated with a previous meniscectomy for an irreparable meniscus tear. The limited surgical indications and the complexity of such operations are the main reasons for the lack of long-term FU studies. Sekiya et al.,17 in their retrospective study, evaluated 28 patients who underwent ACLR with patellar tendon graft (19 patients as primary ACL and 9 patients as revision ACL) with concomitant MAT. They reported substantial improvement in the 36-Item Short Form Survey (SF-36), Lachman and Pivot shift scores and high levels of function during activities of daily living in 90% of patients at an average follow-up of 2.8 years. Yoldas et al.,23 in a group of 31 patients (11 with isolated MAT and 20 with combined MAT-ACLR procedure), compared the outcomes of combined MAT and ACLR with those of isolated MAT. No statistically significant difference emerged between the two groups at a mean follow-up of 2.9 years. Conversely, Rueff et al.24 compared the outcomes of 8 patients undergoing combined ACLR and medial MAT with those of 8 patients who underwent ACLR without MAT at a mean FU of 5 years. Comparable results were observed in terms of VAS Knee Pain, subjective IKDC scores and Lysholm scores. Concomitant lateral and medial MAT in combination with ACLR have also been reported. Zhang et al.,25 in their case report, described the case of a 22-year-old male who underwent medial and lateral MAT after ACLR surgery and subtotal medial and lateral meniscectomy. The procedure restored knee stability and reduced knee pain with an increased level of function at the 30-month follow-up. Baldairon et al.21 reported good short-term functional and anatomical outcomes in five patients after single-stage arthroscopic bi-meniscal replacement by an allograft and/or substitute, with or without concomitant ACLR. Although some studies have shown clinical improvement for combined treatment, data on return to sport remain controversial. Saltzmann et al.,14 in a cohort of 40 patients, found that athletes undergoing lateral meniscus transplantation tended to have higher RTS rates than those receiving medial meniscus transplantations (57% vs 15%, respectively), although this finding was not statistically significant. Zaffagnini et al.,20 in a cohort of 50 patients, reported a return to sport rate of 85% at the final follow-up (mean 5 years). Thirty-nine (85%) patients were able to perform sports activities, and 17 (37%) returned to the same or higher level of sports than before the injury. Although sports practice is generally contraindicated after MAT, especially when involving contact and knee rotations, data on the RTS, which emerge from the present review are encouraging.14 Data on clinical failure rates should not be overlooked. Grassi et al.9 in their case series of 324 patients undergoing MAT, showed that the presence of concomitant cartilage procedure (odds ratio, 0.16; P = .001) and ACLR (odds ratio, 0.40; P = .059) were predictors of failure. The percentage of patients undergoing a re-operation is a number to be considered, even if not always correlated to a surgical and clinical failure. Although the notable findings, the present study has some relevant limitations. Firstly, it is based on a few studies with a small number of patients, with no control group in most of the cases and mid-term follow-up. This may be a bias when attempting to understand the precise role of this combined procedure at long-term FU. Secondly, several data from the available studies were extrapolated using a standardized procedure to minimize errors, but it must be emphasized that the heterogeneity of these studies makes our work subject to bias. For example, different grafts have been used for ACLR and different techniques were used for MAT.
CONCLUSION
MAT combined with ACLR procedure is a viable option in patients with torn ACL and initial chondral damage because of total or subtotal meniscectomy. At mid-term follow-up functional outcomes are satisfactory, the RTS is good and the complication rate is moderate. Further studies are needed to assess the long-term outcomes.
ABBREVIATIONS
ACL: Anterior cruciate ligament
ACLR: Anterior cruciate ligament reconstruction
IKDC: International Knee Documentation Committee
MAT: Meniscal allograft transplantation
RTS: Return to sport
ACKNOWLEDGMENTS
The authors have no acknowledgements
Authors’ Contributions
DC and GC wrote the manuscript and designed the study. FC, LC, MM, VB collected the data. DAS, GM, and SC are the senior authors who reviewed the manuscript. In addition, GC and KC provided data analysis. The authors approved the submitted version.
Disclosures
The authors have nothing to disclose
Conflict of Interest
The authors declare no potential conflict of interest
Funding
None
Informed consent
Not applicable