INTRODUCTION
Partial tears or ruptures of the patellar tendon are a progression of chronic patellar tendinopathy,1 which present similarly and are not as well studied in isolation. The pathophysiology of tendinopathies is complex and multifactorial, but one proposed mechanism involves tendon degeneration and microtears.1–3 Patellar tendinopathy, often also called “jumper’s knee,”4 is a relatively common injury among athletes of sports which involve significant jumping.5–7 Previous studies have estimated an overall prevalence of about 14% in elite athletes across several sports, with a higher rates in elite volleyball players (44.6%) and elite basketball players (31.9%).6 The prevalence was estimated to be lower in nonelite athletes, around 8.5%, and most commonly appearing in volleyball, handball, and basketball.7 These sports share common risk factors for patellar tendinopathy and partial tears, including tall stature athletes, higher body mass, frequent jumping, and hard surfaces.5,8,9 In addition to extrinsic factors, such as tendon overload and overuse,8–11 there is data to suggest that intrinsic factors, such as muscle tightness, muscular imbalance, and malalignment,10,12 may also be contributing risk factors.
Partial patellar tendon tears (PPTTs) present added complexity over patellar tendinopathy and complete patellar tendon tears, as continued sports involvement worsens the damage seen in typical tendinopathy, but a partially intact tendon allows additional treatment options compared to full ruptures.13 Whereas treatment for patellar tendinopathy is generally non-operative,10 treatment decisions for PPTTs are complicated by the severity of the tear, the patient’s preferences, and the goals of rehabilitation.13 Examples of non-operative interventions for PPTTs typically include anti-inflammatory medications, physical therapy, and bracing; however, platelet-rich plasma injections and extracorporeal shock wave therapy have become increasingly popular.13
To date, there is no systematic review summarizing the effectiveness and safety of different treatment modalities, outcomes, and return to sport (RTS) rates for PPTT in athletes. This article aims to provide a comprehensive and updated systematic review of the literature on PPTT in athletes, covering treatment options, outcomes, and RTS guidelines. This article also discusses the challenges and limitations of existing studies and suggests directions for future research.
METHODS
Literature & Database Search
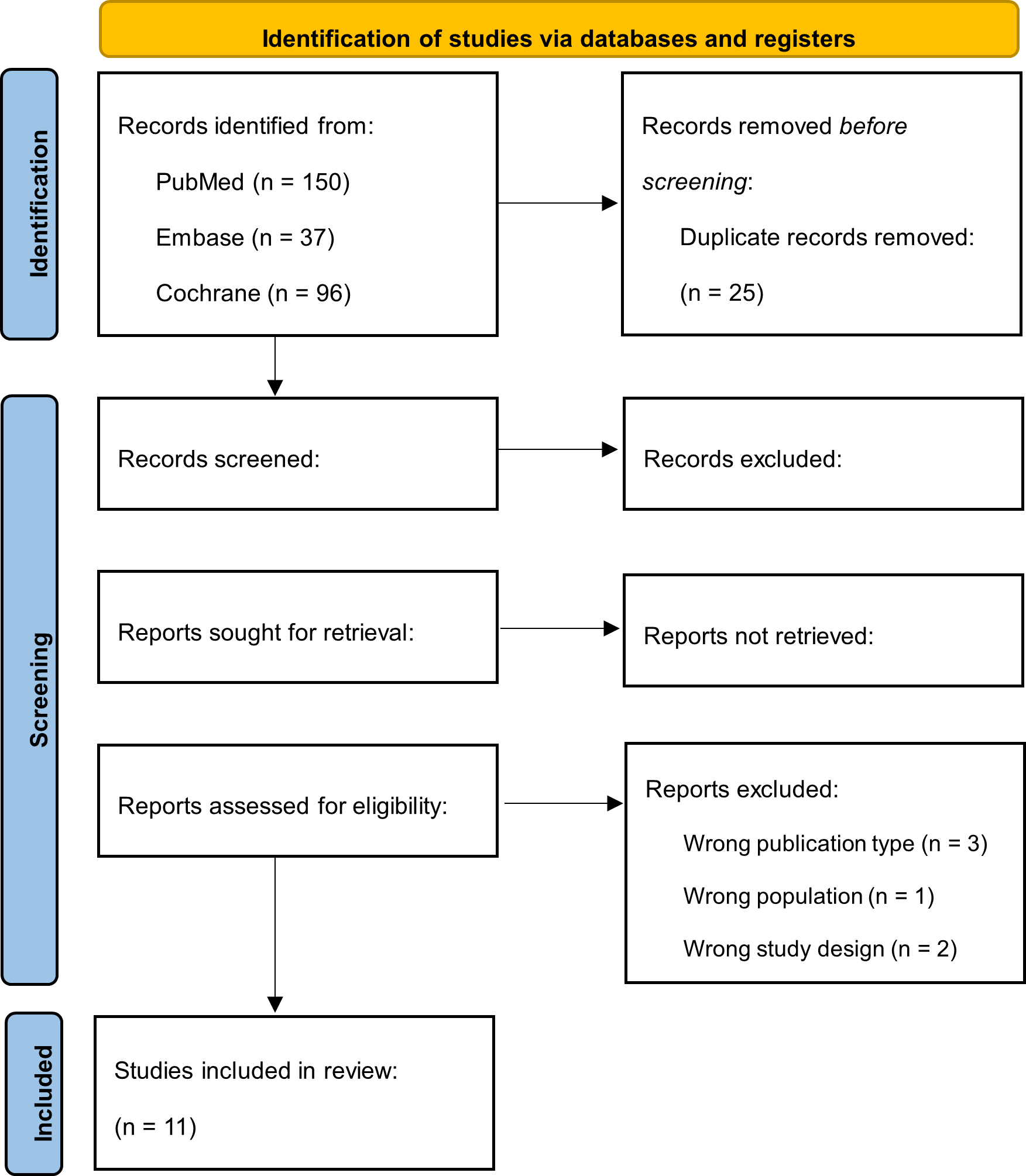
A systematic search of published, peer-reviewed literature was conducted with a research librarian of PubMed (Ovid), Embase (Ovid), and Cochrane from inception of the database to May 1st, 2023. The search consisted of a combination of keywords and controlled vocabulary for the following concepts: partial patellar tendon tear, athletes, surgery, conservative management, treatment outcomes, return to sport. The full details of the search strategy for PubMed, Embase, and Cochrane are available in Appendices A, Table A.1, A.2, and A.3, respectively. All identified records were imported into Covidence reference management software (Covidence, https://covidence.org/) and duplicate references were removed (Figure 1). The literature search and subsequent review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) reporting standards.14

Inclusion Criteria & Study Selection
Two blind reviewers (LS, CR) manually screened titles and abstracts to identify records which primarily investigated partial patellar tendon tears and return to sport (RTS) outcomes in athletic patient populations (Figure 1). Studies which lacked treatment outcomes after PPTTs for athletes were excluded from analysis. Case reports, case series, cohort studies, and randomized controlled trials published prior to database search were included for evaluated for inclusion; however, abstracts, reviews, technical notes, letters to the editor, and surgical technique papers were excluded from evaluation. In addition, cadaveric, non-human, and non-English studies were excluded. Any discrepancies and conflicts between reviewers during the study selection process were resolved by a third, independent reviewer (JS) as needed. The full details of the protocols for this systematic review were prospectively registered on PROSPERO and are available at https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42023416787.
Risk of Bias & Quality Assessment
The risk of bias for included studies was assessed using the JBI Critical Appraisal tools for cohort studies, case series, and case reports.15 Each checklist is comprised of a unique set of questions to evaluate the validity of methods, quality of analysis and presentation for each study type. Two reviewers (LS, CR) each reviewed the included studies and discussed discrepancies to reach a consensus. Any disagreements were settled by a third, independent reviewer (JS).
Data Extraction
For each included study, one reviewer (LS) independently extracted data into a spreadsheet. After a first pass of the studies, the extracted data was evaluated by another reviewer. Any discrepancies and conflicts between reviewers during this process were resolved by a third, independent reviewer (JS) as needed. Extracted data points included: study type and level of evidence, number of patients, male to female ratio, mean age, sport, level of sport, treatment type/modality, follow-up duration, surgical complications, surgical failures/reoperations, RTS, postoperative RTS time, and patient-reported performance outcome measures.
Statistical Analysis
Categorical variables were summated and presented as total counts or proportions, whereas weighted means were calculated for continuous variables. Outcomes of interest were then tabulated in order to highlight the outcomes from individual reports. A meta-analysis was not performed, and individual participant data was not collected.
RESULTS
Literature Search & Screening
An initial search of the PubMed, Embase, and Cochrane databases returned 258 studies, after removing duplicates (Figure 1). Titles and abstracts were initially screened against the inclusion and exclusion criteria, after which 17 studies remained. The full texts of the remaining studies were then screened, where an additional 6 studies were excluded. Data extraction was performed on 11 studies, which comprised 3 prospective cohort studies (Level II evidence), 3 retrospective cohort studies (Level III evidence), 3 case reports (Level IV evidence), and 2 case series (Level IV evidence). All results were reported in conformity with the PRISMA reporting standards.14
Methodological Assessment & Risk of Bias
The included studies were evaluated for methodological quality and risk of bias in accordance with the JBI Critical Appraisal tools for cohort studies, case series, and case reports.15 Three prospective cohort studies16–18 had a mean score of 9.3 out of 11. Three retrospective cohort studies13,19,20 had a mean score of 9.7 out of 11. Three case reports21–23 had a mean score of 8 out of 8. Two case series24,25 had a mean score of 9.5 out of 10. All studies were deemed suitable for inclusion for this review based on the JBI Critical Appraisal tools criteria.
Patient Demographics
The 11 studies included in this review featured a total population of 454 patients, comprised of 343 males (86.2%), 55 females (13.8%), and the remaining unknown due to unclear reporting in one study (Table 1). The weighted average age of the patients in the included studies is 25.84 years, with a range of 15 to 55 years. There was a diverse set of sports reported by the patients, including: volleyball (n=60), soccer (n=49), running (n=45), basketball (n=36), jumping (n=28), sprinting (n=13), body building (n=11), decathlon (n=9), baseball (n=8), javelin/shotput/discus (n=8), football (n=7), tennis (n=5), tennis/squash/ski (n=5), European handball (n=4), gymnastics (n=3), jai alai (n=1), and lacrosse (n=1). Two studies did not quantify the specific sports practiced by participants.16,18 The level of sport was varied and inconsistently reported across studies; therefore, subjects were grouped into elite and non-elite. Elite athletes were defined as athletes who compete professionally or at national levels, while non-elite included all other athletes.11 Five studies provided level of sport data, of which two included elite athletes24,25 and three included non-elite athletes.19,22,23 Six studies did not specify the level of sporting for the participants.
Treatment Options & Complications
Both operative and non-operative treatment options were used in the treatment of PPTT injuries (Table 2). A total of 169 patients (37.2%) received only conservative, non-operative treatments.13,16,18,21–23 These regimens included physical therapy, immobilization, shock wave therapy, and/or ultrasound-guided platelet-rich plasma (PRP) injection. Only one study specified the PRP injection type used, the PRO-PRP KIT leukocyte-poor platelet-rich plasma.23 There was no available data in these studies comparing the efficacy of different non-operative treatments. In contrast, a total of 295 (65.0%) of patients were treated surgically.13,16–20,24,25 Most of these patients had undergone surgical repair after failing to improve with conservative management. Surgical approaches generally consisted of debridement only16–20 or debridement with anchors,25 with one study reporting both techniques13 and one study not specifying the technique used.24 Only one study reported surgical complications, where 2 patients developed superficial wound infections.18 Reoperations were reported in 20 patients (6.8%) across several studies. Patients were followed for a mean duration of 55.8 months. Post-operative physical therapy was described in several studies: five studies described progressive range of motion rehabilitation (with or without bracing) followed by isometric and/or isokinetic strengthening exercises,17,18,20,25 one study described isometric strengthening alone,19 and three studies did not elucidate a post-operative physical therapy regimen.13,16,24 One study provided a detailed outline of the physical therapy program used to rehabilitate patients post-operatively: After 4 weeks of immobilization in a long leg cast, patients began a daily training program consisting of progressive overload exercises including knee extension and leg press exercises. The program also included dynamic exercises such as bicycling (50-300 Watts), walking/jogging on soft mattresses, stair/obstacle walking, and (later) jumping activities.18
Treatment Outcomes & Return to Sport
Return to sport was defined as a return to general sporting activity, irrespective of pre-injury performance level. RTS was seen in 267 patients (92.1%) after PPTT treatment, with an average postoperative time to RTS of 3.9 months (Table 2). A direct comparison of RTS rates between operative and non-operative patients was made in one study, with 7 of 11 (63%) and 40 of 45 (89%) returning to previous levels of activity.13 Three studies19,21,25 included range of motion (ROM) data. In addition, other outcome measures that were available included: Lysholm’s knee score,26 Victorian Institute of Sport Assessment (VISA) score,27 Blazina scale,4 and Cybex II dynamometer measurements.28 One study19 collected data on postoperative pain as compared to the preoperative state, with patients generally reporting improvements in their pain postoperatively.
DISCUSSION
The objective of this systematic review was to evaluate treatment outcomes and RTS in athletes with PPTT injuries. A review of 11 studies found a 92.1% RTS rate in treated patients. On average, athletes were able to RTS after 3.9 months of treatment. Patients who received operative treatment represented 65.0% of the sample, while patients who only received non-operative treatment represented 37.2% of the sample. Many of the operatively treated patients had failed to improve with previous non-operative treatments. Reoperations were reported in 6.8% of cases. On average, the patients were followed for a duration of 55.8 months.
A comparison to full-thickness (“complete”) tears of the patellar tendon reveals that the RTS rate for complete patellar tendon tears is significantly lower, as reported in studies of professional basketball (75%) and football (50%) players.29,30 In non-elite players, one study on complete patellar tendon tears reported a RTS rate of 87%, which was closer to, but still below, the RTS rate we found in PPTTs.31 Similarly, athletes treated for a PPTT showed a higher RTS rate than patients treated for an anterior cruciate ligament (ACL) tear, where RTS rates ranged between 69% and 87%.32–35
Across the studies examined, PPTT treatments generally began with conservative measures, especially physical therapy, immobilization, injections, and symptom management.13,18,21–23 Only one study18 detailed the physical therapy program used for patients; further research is needed to establish a consensus on the best physical therapy protocols. In some of the studies,13,16,18 this conservative approach was insufficient for some patients and resulted in escalation to surgery. This explains the much larger number of operative patients (65.0%) as compared to solely non-operative patients (37.2%). While there are no studies which directly compare the operative and non-operative treatment outcomes, the data from these studies showing that non-operative treatment is insufficient for certain patients suggests that there may be a relationship in the characteristics of a PPTT and the optimal treatment approach.
Golman et al.13 analyzed the relationship between tendon tear thickness and progression to surgery and found that all patients in the study who required surgery had tears of greater than 50% thickness; this suggests that non-operative therapy is less effective for patients with more severe tears and would benefit more from an operative approach. Interestingly, they did not find any correlation between the severity (i.e., size or percentage) of tear and RTS. The data and novel PPTT classification system these authors present may facilitate more uniform and evidence-based treatment approaches; however, further studies are needed in this area.
The reoperation rate for this sample of patients was reasonable in the context of similar knee operations. We reported a reoperation rate of 6.8%, which was slightly lower than the revision rate for ACL reconstructions. Several cohort studies have reported ACL reconstruction revision rates between 7.1% and 16%.35–37 Screw removals and meniscus procedures were the highest represented causes for reoperations and revisions after primary ACL reconstructions.35,36 Similarly, a 9.9% reoperation rate in acute, complete patellar tendon tear reconstructions is lower than our findings for PPTT operations.38 In acute patellar tendon tears, retears, adhesion lysis, and wound debridement represented the most common causes for reoperation.
The studies in this review reported various postoperative RTS times, as shown in Table 2. With a range that varied from 2 months to 6 months, many of the studies framed RTS capability on the basis of individual performance measures. It is important to make considerations for the sport and the level of sport in an athlete when making RTS recommendations. In addition, more objective performance measures are important to guiding RTS. For example, Karlsson et al. (1991) specified “that patients should not return to sports activities until both the quadriceps and hamstring strengths are over 90% of that of the uninjured side.”17 However, the severity of tear may not be a useful factor in making RTS recommendations, as was explained above.
This review was limited primarily by the variety of methods used to measure treatment outcomes. The heterogeneity of available data complicates comparisons across studies. For example, only one study21 provided specific ROM data, while two other studies19,25 provided qualitative comparisons of ROM and strength between injured and non-injured legs. Two studies18,20 reported data as either the number of patients or the number of knees affected, which differed as some patients presented with bilateral injuries. Therefore, many of analyses did not include the total patient population. Another limitation of this review is the lack of individual patient data. Lastly, the treatment outcomes in surgically treated patients may be confounded by differences in surgical techniques, which have likely improved over the 30 years represented in this data.
CONCLUSION
A PPTTs is an injury amongst athletes participating in sports with frequent jumping, such as volleyball or basketball. This systematic review analyzed 454 athletic patients in 11 studies, spanning from 1991 to 2021, and illustrates return to sport rates over 90% following conservative or surgical treatment. Many patients first attempted non-operative treatments and were operated on after failing to improve with prolonged conservative management. The patients who underwent surgical treatment had a lower reoperation rate than comparable surgically treated knee injuries. The high RTS rate and low reoperation rate in surgical cases suggests that current treatment options are satisfactory; however, there is currently little data that directly compares the treatment options to establish a superior treatment modality. While the data we present suggests that current treatment options are largely successful, further comparisons are needed to the most effective treatment options.
Acknowledgments
None.
Conflict of Interest
None.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
AUTHOR CONTRIBUTIONS
Luke A. Sandoval: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Validation, Visualization, Writing – original draft, Writing – review & editing. Charles R. Reiter: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Validation, Visualization, Writing – review & editing. James Satalich: Conceptualization, Investigation, Methodology, Project administration, Supervision, Validation, Writing – review & editing. Conor O’Neill: Conceptualization, Investigation, Methodology, Project administration, Supervision, Validation, Writing – review & editing. John Cyrus: Data curation, Investigation, Methodology, Resources, Software, Writing – review & editing. Robert O’Connell: Conceptualization, Investigation, Methodology, Project administration, Supervision, Validation, Writing – review & editing. Alexander Vap: Conceptualization, Investigation, Methodology, Project administration, Supervision, Validation, Writing – review & editing.