Introduction
Total joint replacement (TJR), also referred to as replacement arthroplasty surgery, is performed on patients with impaired joints that cannot be nurtured by non-invasive means. Impaired joints are usually the result of arthritis, prior fractures, injuries to the specific joint, or other diseases.1 One of the leading causes of TJR is osteoarthritis.2 Osteoarthritis is a process that causes a loss of articular cartilage and creates focal erosions that traverse the bone and affect the surface of the joint.3 OA is the most common form of arthritis and is associated with BMI, as indicated by a study done on obesity and OA (OR: 1.65; 95% CI: 1.46-1.87, P<0.001).4 Furthermore, it is a disease that is significantly associated with age.3 Patients, for the most part, have positive outcomes with TJR, but a study done in 2018 reported that 20% of patients were unsatisfied with their total knee replacement (TKR). One of the most common pre-operative predictors of dissatisfaction was pre-operative anxiety or depression.5 Furthermore, little is known about how post-discharge care experience and financial status can impact the patient’s overall satisfaction rating.6
In this study, we aimed to find factors influencing patient satisfaction with TJR in the United States (US). Patients’ concerns with their replacement arthroplasty surgery include postoperative complications, mobility, and pain management. The fiscal status of the patient, including insurance type and costs of the surgery, are factors that influence patient satisfaction as well.7 Due to all of these variables, many patients, although it would benefit them tremendously, refuse to take the procedure to better their arthritis.8 Amongst TJR procedures, studies have shown that total knee arthroplasty is currently one of the most successful surgeries, with a success rate between 90% and 98%.9 Yet, some patients are hesitant to undergo this procedure or remain unsatisfied with their care throughout the process. Our goal in this study was to determine which specific factor or multitude of variables had the largest impact on patient satisfaction.
Methods
An anonymous web-based survey was conducted for patients who had undergone any total joint replacement surgery, including hip, shoulder, and knee, in the US. The survey began with a screening question that required patients to select whether they had a hip, shoulder, or knee replacement from a list of surgical procedures to participate in the study. The survey then consisted of multiple choice questions asking about their pain and mobility levels before and after the surgery. Free response questions (FRQ) asked participants about their ability to pay for surgeries and out-of-pocket physical therapy, rehabilitation, and medication costs. In addition, another financial question was asked whether or not the patient added difficulty paying for the following: surgery, rehab/physical therapy (PT), and or medications. Postoperative complications were also assessed in the survey, along with overall satisfaction with the surgeon. JMP Pro 15 statistical software was used to analyze and visualize the data.
Results
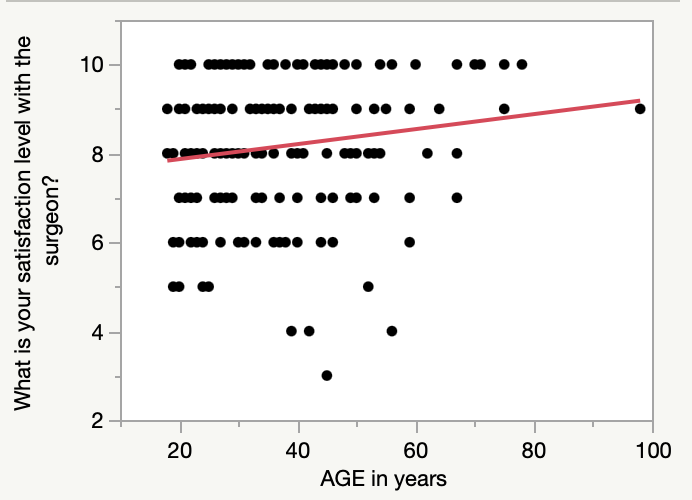
Our study included 180 participants who met the inclusion criteria and responded to the survey. Distribution of surgery type consisted of 64% of the cohort selecting knee surgery, while only 21% and 14% accounted for the people who selected shoulder and hip surgery. Age, education, gender, and race were fitted against reported patient satisfaction levels with the surgeon. While education [P=0.47198], gender [P=0.50972], and race [P=0.81831] were not significant, age in years [P=0.02340] was predictive of overall satisfaction levels [R2=0.0213]. A logistic regression fit visualizes this relationship below (Figure 1).

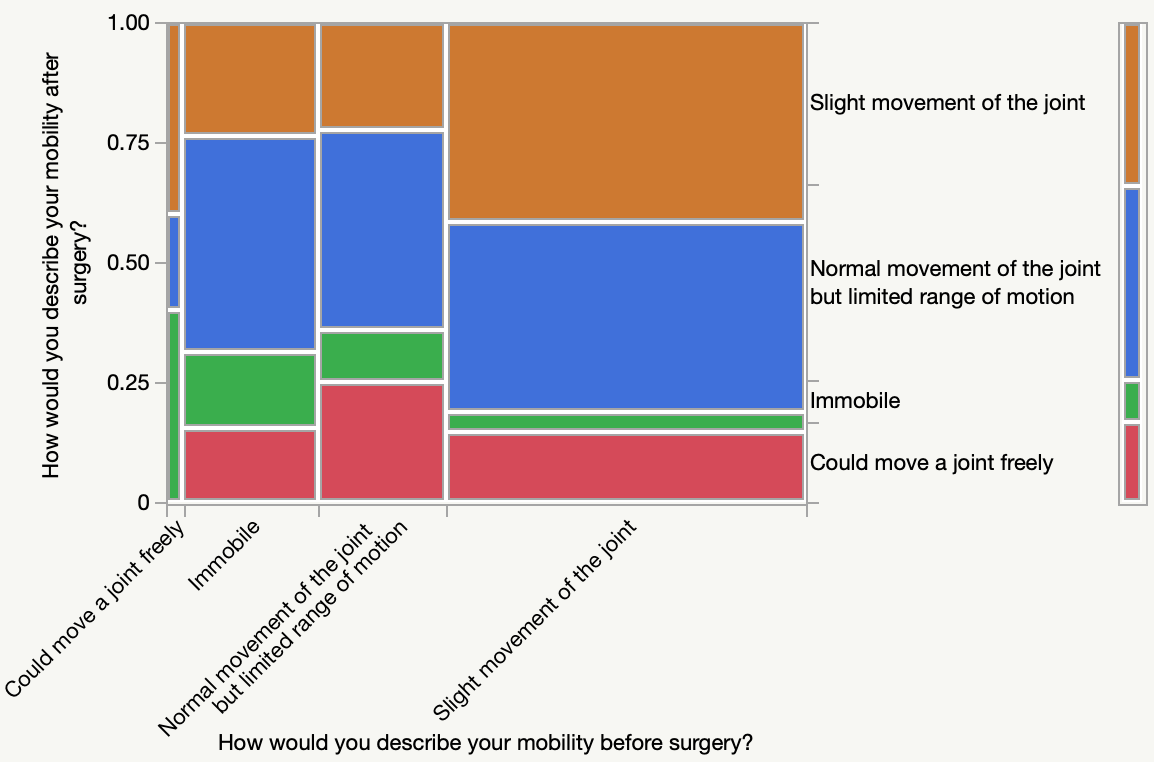
When controlling for basal metabolic index (BMI), infection [P=0.0164], nerve damage [P=0.0250] (Figure 3), delayed healing [P=0.0024] (Figure 4), and hematoma [P=0.0497] were more likely to occur in participants who have had a knee replacement, but this was not true or significant for shoulder and hip replacement surgeries. When comparing mobility levels before and after surgery, patients who reported higher levels of mobility before surgery were also more likely to select higher levels of mobility after surgery in the survey [P=0.0114] (Figure 2).

Insurance types were fitted against patients’ self-reported difficulty in paying for their treatment/care. Although employer-based insurance [P=0.0790] was not significant, Medicaid [P=0.0280], Medicare [P=0.0200], and private insurance [P=0.0343] were predictive of overall patient self-reported difficulty in paying for their treatment/care.
Discussion
In the cohort, patients of older age were found to have higher satisfaction levels with the surgeon who performed their joint replacement surgery as compared to younger patients. Another study also found that satisfaction with knee replacement surgery was the greatest in older patients - wherein 86% of younger patients and 91% of older patients reported feeling satisfied with their care.10 Furthermore, the overall quality of life among older patients was greater than that of younger patients. Although younger patients had higher levels of self-reported activity before and after their procedure, they experienced more knee-related dissatisfaction. In our study, it was found that regardless of knee, hip, or shoulder surgery, lower levels of satisfaction were associated with younger patients. This could be due to older patients sustaining a degenerative joint disease for many years, which entails that they might have lower expectations of experiencing pain relief after their procedure.11 Additionally, younger patients who could be accustomed to a more active lifestyle may have higher expectations for the success rate of their arthroplasty surgery compared to older patients, leading to more dissatisfaction among younger patients if the surgery doesn’t have high success rates.12
Throughout this study, affordability has been a significant factor in our evaluation of patient satisfaction with their TJR. This variable is also represented in another study that focused on how belonging to a low-income bracket and using public insurance, like Medicaid, can result in the inability to afford and access health care.13 This finding is also consistent with a systematic review that states that insurance type and socioeconomic status have a significant impact on patients’ access to total joint arthroplasty (TJA).14 Both of these studies agree with our data and claims regarding affordability with TJR. It can be concluded that public-based insurance can cause a patient to have a difficult time paying for their TJR procedure. This could be due to public-based insurance not covering the entirety of the surgery and forcing out-of-pocket (OOP) costs for the patient.15
In this study, patients who reported higher levels of mobility before surgery were also more likely to select higher levels of mobility after surgery in the survey. However, another study refutes this claim as their study portrays that knee arthroplasty patients with pre-operative motion below 90 degrees improved 26 degrees more than patients with a pre-operative motion greater than 105 degrees.16 In their study, they focused on the range of motion before and after a knee arthroplasty procedure and measured flexion to determine how different degrees of motion fare with each other. Although this study slightly disagrees with our data, there is an indication of both studies not directly being connected. Our study found that no other levels of pre-operative mobility were predictive of post-operative mobility levels, so we can’t make the claim that patients with lower levels of mobility before the procedure had less range of motion after the surgery than patients with higher levels of mobility before the surgery. However, other literature has proven that early mobilization tends to lead to a reduced risk of postoperative complications, accelerates reinstitution of walking capacity, and has positively affected several patients’ reported outcomes.17 This was a finding equally represented in our data.
Other studies that have been done on patient satisfaction with TJR include different aspects of focus ranging from country to timeline of observance. The first study was able to develop a study that observed TJR patients for five years, allowing for more data that could be helpful in determining which factors had the largest impact on patient satisfaction with TJR.18 An analysis of patient satisfaction with total hip arthroplasty honed in on a Japanese cohort, differing greatly from this cohort.19
There are several limitations to the current study. First it comprises several joint replacements, including shoulder, knee, and hip and this diversity of joints potentially makes the data harder to interpret. For example, mobility may be more impacted by lower extremity joint replacements compared to a shoulder replacement. This in turn could impact satisfaction. Further, the survey did not have a question establishing overall satisfaction, only satisfaction with the surgeon. . Another limitation would be the distribution of the surgery type variable. After reviewing the distribution in the study, 64% of the cohort selected knee surgery, while only 21% and 14% accounted for the people who selected shoulder and hip surgery. This could have greatly affected the data found when controlling for BMI and surgery type vs. post-operative complications. Since more participants selected knee surgery, that could mean that more people selected post-operative complications for knee surgery specifically rather than being an indicator for all post-operative complications. One limitation that was especially accounted for was recall bias, as it was specifically established in the screening question stating that the participants must have undergone the TJR surgery in the past year to meet the inclusion criteria.20 This ensures a perfect timeline for the patient to remember their surgery and experience.
Conclusion
In this sample, a patient’s age was substantially associated with higher satisfaction with the joint replacement surgeon. Older participants would select satisfaction levels anywhere from 8-10, but younger participants would select satisfaction levels anywhere from 5-7. Patients who got knee arthroplasty surgery experienced more complications than those who underwent shoulder or hip arthroplasty. Furthermore, when looking at the financial aspect of the study, we found that most patients had one of the following insurance: Medicaid, Medicare, and private insurance. In addition, patients who reported difficulty regarding affordability with their care had these insurances. This indicates that patients’ ability to pay for treatment, surgery, and medicine was difficult when having government-based insurance.