Introduction
Total Knee Arthroplasty (TKA) is one of the most frequently performed orthopedic procedures and is projected to grow to 935,000 annual procedures in the United Sates by 2030.1 Despite being a common orthopedic procedure, up to 20% of patients remain dissatisfied with their outcome.2 This dissatisfaction may due to intrinsic or extrinsic causes and is often described in terms of pain, stiffness, instability, or a combination of these.3,4 Severity, timing, associated symptoms, and – for the purposes of this review – location of that pain can all aid the orthopaedic practitioner in developing a focused differential.
Well described etiologies for a painful knee following total arthroplasty include infection, component malposition, components oversized, inadequate soft tissue balancing, hardware failure, periprosthetic fracture, instability, aseptic loosening, polyethylene wear, arthrofibrosis, patellar maltracking, patella baja, patella overloading, patella avascular necrosis, irritation of the infrapatellar branch of the saphenous nerve, and hypersensitivity to implants.3,5–7 These source of pain should be considered in every patient who presents with persistent knee pain. Initial strategies detailing appropriate history, exam, studies, and laboratory markers have been well described.3,4
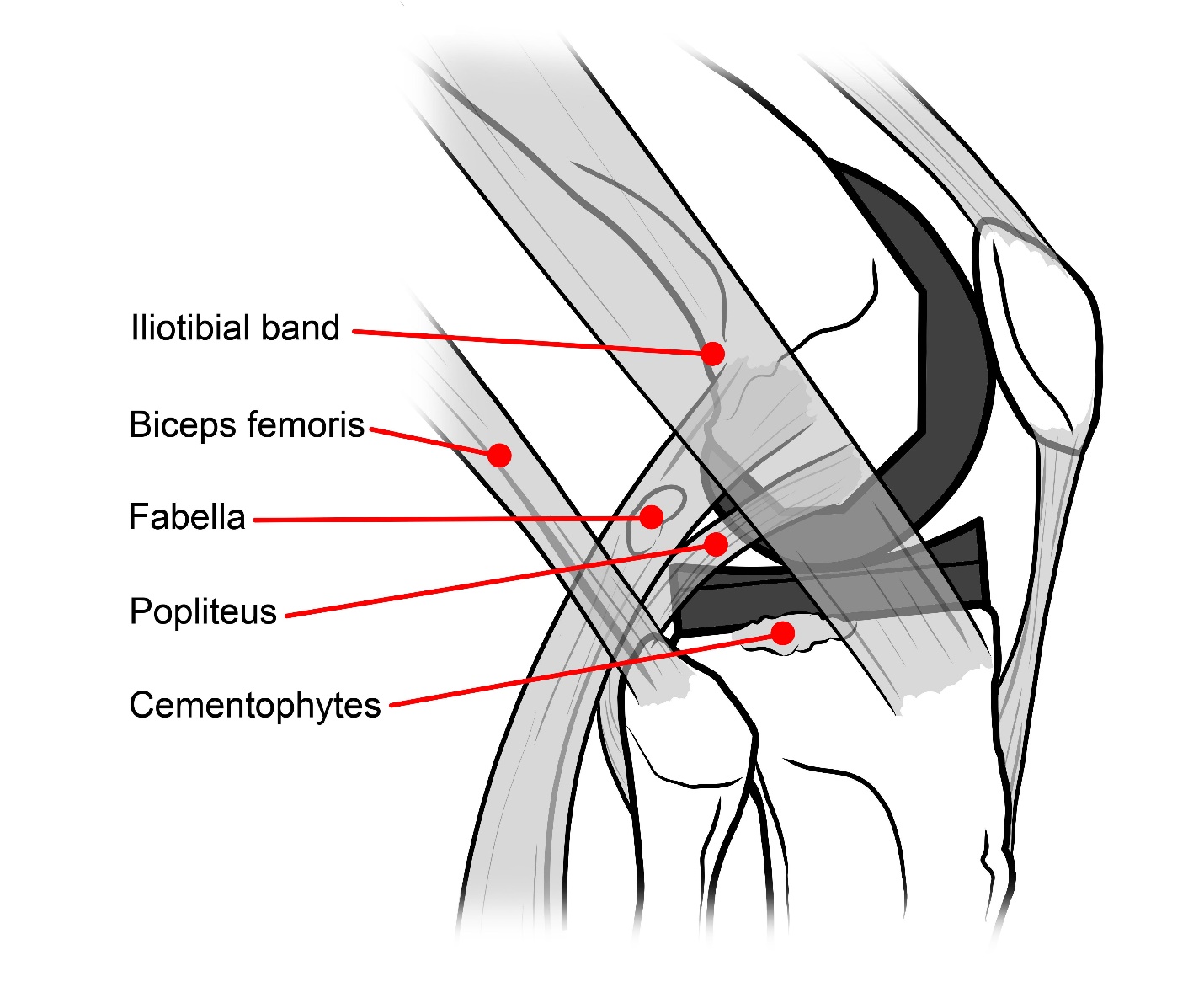
Localizing pain is an important part of the initial evaluation, and patients will most commonly describe pain in multiple areas.7 Isolated pain is much less common, but if the patient attributes their pain to a single specific anatomic location, this can help suggest the source of the underlying problem. Anterior knee pain is the most common area of pain and many reviews have investigated the causes of anterior knee pain.7–11 Isolated lateral sided knee pain is rare but concomitant lateral sided pain has been reported 63% of patient who are unhappy after a TKA .7 As such, practitioners must have a working knowledge of specific sources of lateral sided knee pain to ensure comprehensive management. The purpose of this study is to present a detailed literature review evaluating the unique causes, diagnoses, and management strategies for addressing isolated lateral-sided knee pain after TKA. These include Iliotibial Band Friction Syndrome (ITBFS), Iliotibial Band Traction Syndrome (ITBTS), biceps tendinitis, fabella syndrome, popliteus tendon impingement, and impingement of synovial tissue (Table 1, Figure 1).

Iliotibial Band Friction Syndrome
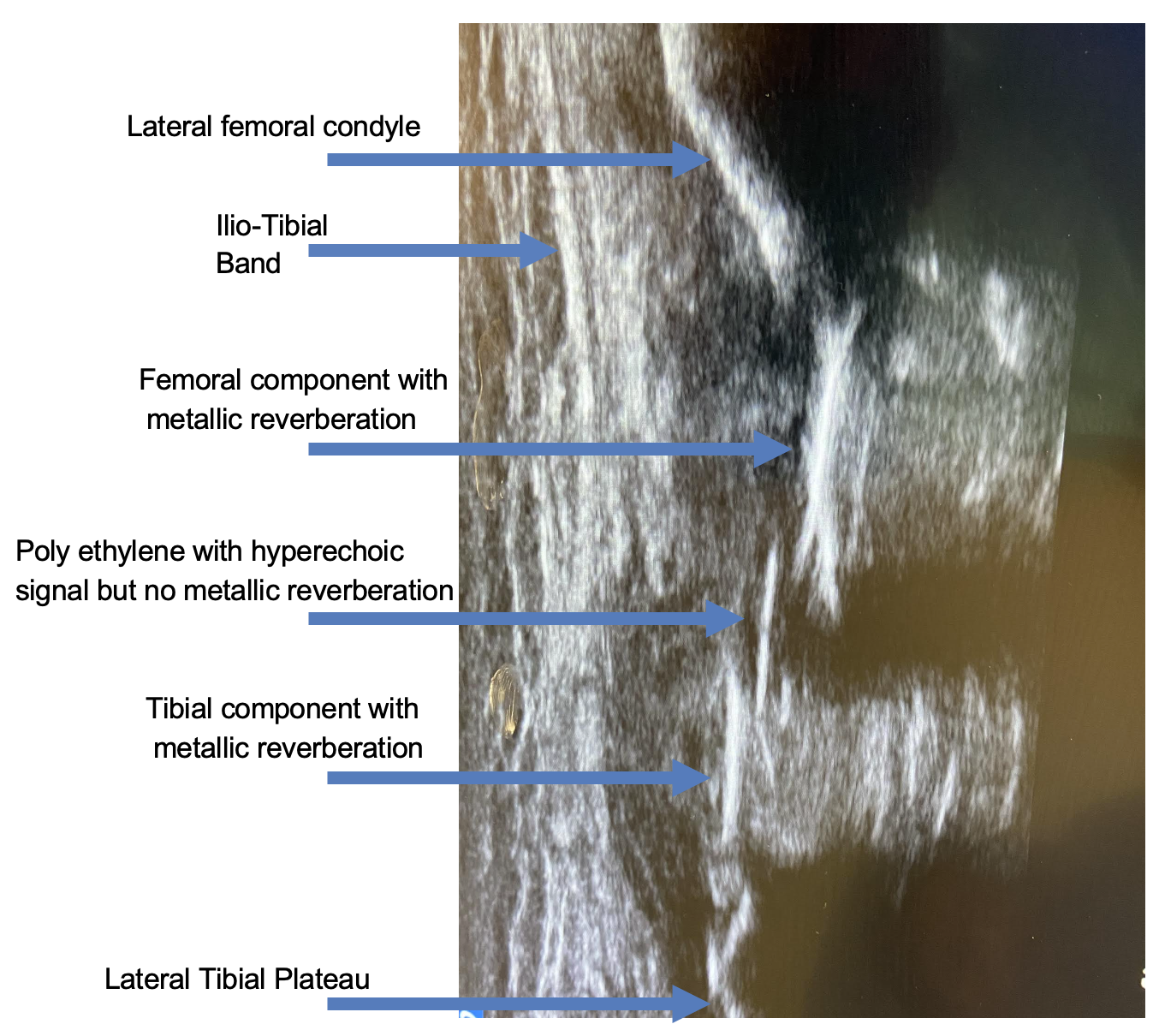
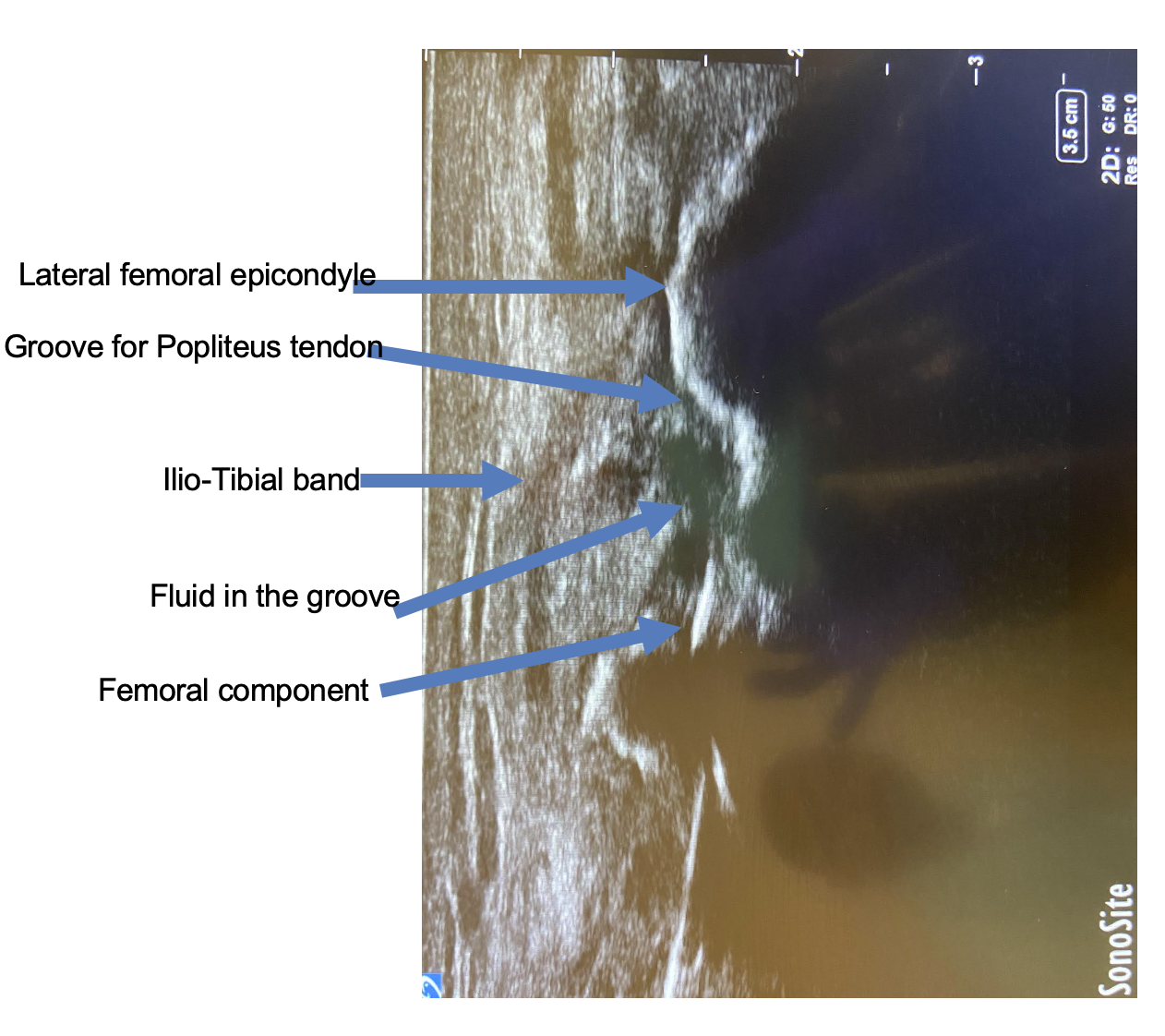
Iliotibial band friction syndrome (ITBFS) is a well described cause for isolated lateral-sided knee pain after TKA. While debate persists regarding the exact etiology of pain in the native knee, in patients having undergone TKA, irritation of the iliotibial band (ITB) against an underlying prominent structure including unresected osteophytes, cementophytes, and misaligned or overhanging implants has been demonstated.12,13 Patients may present with localized tenderness along the ITB and palpable crepitus secondary to the soft tissue gliding across the underlying prominence. Radiographic evaluation including plain films and computed tomography (CT) can identify sources of impingement. Ultrasound guided local anesthetic injections can aid precision of diagnosis (Figure 2 and 3). Treatment is dependent upon the etiology. In the setting of extruded cement or any unresected osteophytes, treatment involves removal and possible partial release of the ITB at the level of crepitus or tenderness.13 ITBFS caused by lateral overhang of the tibial tray can be primarily avoided by palpating the lateral cortical rim while sizing the tibia.7 However, in some TKA systems, the tibial component sizes are limited by the femoral component size, which may compromise the ability to downsize the tibial component to avoid overhang. Special care and planning must be taken when using such systems. In a case report, Kwok et al. describe the lateral overhang of a tibial tray by 3mm which caused localized pain and tenderness at the ITB insertion at Gerdy’s tubercle.14 The patient was successfully treated with arthroscopic excision of the impinging portion of the ITB. The fascial defect was not closed to allow soft tissue remodeling. This patient was followed up for three years without any complications and no recurrence of symptoms. The authors recommend combining the arthroscopic approach and open approach to maintain the integrity of the lateral capsule to decrease infection risk.14
.png)
.png)
Iliotibial band Traction Syndrome
Iliotibial band traction syndrome (ITBTS) is a new clinical condition that can occur after the use of a guided motion Bi-cruciate stabilized TKA.5 It is different from other ITB conditions because it is thought to be caused by abnormal stretching of the ITB due to forced guided motion from the implant, which does not allow for natural kinematic variability in native knees. The Bi-cruciate stabilizing (BCS) Knee System was introduced in 2005 to replicate normal knee kinematics, and it is significantly different from most conventional posterior stabilized systems. The BCS Knee System has an anterior cam-post mechanism that engages around 20 degrees of flexion, and a posterior cam-post mechanism that engages around 60 degrees of flexion. The posterior cam is asymmetrical in shape, guiding the femur into external rotation during flexion and internal rotation during extension. This design feature replicates the normal motion of a native knee with intact anterior and posterior cruciate ligaments. This forced guided motion is thought to contribute to increased stretching of the lateral retinaculum, increasing pressure between the lateral femoral epicondyle and ITB causing lateral knee symptoms especially in the mid arc range of motion (ROM) between 200 and 700. Symptoms can be treated conservatively or by surgical release of iliopateallar retinaculum.6,15,16 Diagnostic local anesthetic injection with or without steroids can help to confirm the source of pain and aid in decision making for the surgery. The second-generation BCS knee introduced in 2011 that has changes in design and has decreased incidence of lateral knee pain (1.9%)17 even though occasional cases have been reported.18
Biceps tendinitis
Biceps tendinitis described source of lateral knee pain in native knees, it is an uncommon pain source after TKA. Pandher et al. describe a patient who presented 22 days after his index TKA with acute onset of severe posterolateral knee pain with localized tenderness along the course of the biceps tendon.19 Ultrasonographic evaluation revealing hypoechogenic fluids around the biceps tendon. The patient’s symptoms improved after ultrasound-guided peritendinous lidocaine injections combined with NSAIDS. The pain and tenderness from biceps femoris tendinitis are located more posterior when compared to ITB related pain and more lateral when compared to popliteal tendinitis. Ultrasound is a useful tool to confirm the diagnosis of biceps tendinitis.
Fabella Syndrome
The fabella is a sesamoid bone within the lateral head of the gastrocnemius and is present in 36.8% of the population.20 It is more than twice as common in men and prevalence increases with age.20 The structure articulates with the posterior surface of the lateral condyle can become symptomatic in both native knees and after knee arthroplasty. In the setting of a TKA, it is thought that impingement occurs between the fabella and the posteriolateral edge of the femoral component and/or the posterior edge of the polyethylene component. Fabella syndrome is associated with the insidious onset of posterolateral knee pain, that pain may be localized medial to the biceps femoris.21 Patients may report pain and snapping or clicking sound during knee due to the compression of the fabella against the lateral femoral condyle.21 Length of fabella ≥1.0 cm, incorrect placement of components, and ligament instability have been identified as risk factors for fabella syndrome after TKA.22 This condition may be treated with fabellectomy through a separate posterolateral incision and can be combined with an arthroscopic evaluation of the knee to rule out other intraarticular pathology, especially for popliteus tendon impingement.23
Popliteus Tendon Impingement
Popliteus tendon pain following TKA has been well described and is the result of tendon impingement which may include an excessively lateralized femoral component, overhanging posterolateral tibial tray, or unresected osteophytes.24 In the absence of a clear radiographic cause, dynamic sonography can demonstrate the relationship between implants and neighboring tendons.25 The diagnosis has been made alongside otherwise well sized components, and it is theorized that resection of the menisco-popliteal ligaments during lateral meniscal resection destabilizes the popliteus resulting in impingement against the tibial tray during deep flexion.26 Patients with popliteus tendon impingement report pain and a snapping sensation along the posterolateral aspect of the knee as the knee is flexed and extended. There is discrete tenderness along the course of popliteus tendon at the level of the joint line. The incidence of painful popliteal impingement requiring surgical intervention is unknown but estimated at 2/1000.27 In a series of 300 consecutive TKAs, popliteal tendon snapping was detected intra-operatively in 8 cases (2.7%) and treated with release from the femur.28 However, it is uncertain if all these snapping popliteus tendons would have been symptomatic if left untreated. Relief of symptoms after ultrasound-guided local infiltration with local anesthesia into the popliteal tendon sheath aids in diagnosis (Figure 2 and 3). Non-operative management includes anti-inflammatory medications and physical therapy. If non-operative management fails, arthroscopic release of the popliteus tendon at the femoral attachment has been shown to resolve the pain and no residual laxity has been reported.13–15 In a blinded clinical and cadaveric study, Kesman et al. could not identify the clinically significant intraoperative differences in stability with and without popliteal resection.29 An anterolateral arthroscopic portal usually provides an optimal view, and debridement of the scar tissue along the anterolateral gutter facilitates the visualization of the popliteus tendon. A separate accessory lateral portal is often required to release the popliteus tendon from its femoral attachment.
Synovial Tissue Impingement
Synovial tissue impingement has been described in both anterior and lateral aspect of the knee.30,31 Barr et al. described a patient that underwent a diagnostic arthroscopic evaluation who had isolated lateral knee pain that had negative imaging and failed non-operative management. Intraoperatively it was noted the patient had excessive synovial tissue in the lateral gutter resulting in impingement and synovitis. Imaging is unlikely to identify this abnormality, and so this diagnosis remains one of exclusion. Many authors have demonstrated the utility of arthroscopy to help diagnose patients with pain after knee arthroplasty.32 A recent systematic review of 609 patient who underwent arthroscopy after knee arthroplasty concluded that the procedure is a reliable therapeutic option and cited pain with no clear diagnosis as a top indication for the surgery. In that review, 80% of the patients did not require a later revision.33 However, this use of arthroscopy is not benign and large database inquiries have demonstrated an association with revision for infection.34
Discussion
Lateral side knee pain following total knee arthroplasty (TKA) can be a challenging issue for both patients and orthopedic surgeons. In this context, identifying the source of pain is crucial for effective management. One of the key contributors to lateral knee pain after TKA is Iliotibial Band Friction Syndrome (ITBFS). This condition occurs when the iliotibial band rubs against prominent structures like unresected osteophytes or misaligned implants, leading to localized tenderness and crepitus.12,13 Diagnosis often involves radiographic evaluation and ultrasound-guided injections for precision. Treatment depends on the specific cause, which may involve removing osteophytes or releasing the ITB if it’s impinging on the knee.13 Careful planning during surgery can also help prevent lateral overhang of the tibial tray, which can contribute to ITBFS.14
Another noteworthy cause of lateral knee pain is Iliotibial Band Traction Syndrome (ITBTS), which can occur after certain types of TKAs.5 It results from abnormal stretching of the ITB due to forced guided motion from the implant, particularly in the mid-arc range of motion. This condition can be treated conservatively or with surgical release of the iliopatellar retinaculum, with newer TKA designs showing reduced incidence.15–17
Other potential causes of lateral knee pain include biceps tendinitis, fabella syndrome, popliteus tendon impingement, and impingement of synovial tissue.19,21,24,30 Each of these conditions presents unique challenges and may require specific diagnostic tools like ultrasound (Figure 2 and 3) or arthroscopy for confirmation and treatment. The thorough evaluation and understanding of these causes are essential for orthopedic surgeons to provide comprehensive management and address patients’ persistent lateral-sided knee pain following TKA.
Conclusion
Isolated lateral-sided knee pain after TKA is an unusual cause of pain and soft tissue impingement is a common culprit. Initial work up should include ruling out the most common causes of painful TKA including infection, aseptic loosening, and instability. Radiographs and CT scan are utilized to identify potential source of pain. Ultrasound evaluation (with elicited probe tenderness) can increase diagnostic accuracy. Ultrasound guided local anesthetic injections can confirm the source of pain. Anti-inflammatory medications, physical therapy with ITB stretches, and therapeutic local steroid injections are initial treatment modalities. Satisfactory resolution of symptoms may require surgical intervention directed at the specific cause and may avoid the morbidity associated with revision TKA.