
_postoperative_anterolateral_radiograph_of_the_right_lower_leg_after_the_first_surger.tiff)
_postoperative_anterolateral_radiograph_of_the_right_lower_leg_after_the_second_surge.tiff)

Introduction
The process of bone healing is typically divided into two ways: primary healing and secondary healing,1 with secondary healing being the most common clinical method of fracture healing.2The secondary healing process consists of four stages: acute inflammatory response, fibrocartilaginous formation, bone callus formation, and bone remodeling. Acute inflammatory response typically occurs in the first few days after the fracture, fibrocartilaginous formation usually takes place between 5 to 10 days after the fracture, bone callus formation generally occurs around 4 weeks after the fracture, and bone remodeling typically takes several months to a year to complete.3 During the acute inflammatory response stage, there is a significant presence of hematoma and inflammatory cells at the fracture site. The fracture fragments are unstable. In the fibrocartilaginous formation stage, there is a large amount of fibroblasts, osteoblasts, chondroblasts at the fracture site, and the fracture fragments directly connect and unite as a whole. In the bone callus formation stage, there is a cartilaginous callus at the fracture site, providing basic mechanical stability.4
Locked plate external fixation has been applied in clinical practice since the 19th century.5 Previous studies have primarily focused on the application of locking plate external fixation in the management of open fractures, bone infections, nonunion, and other related conditions.6–9 Compared to traditional external fixation, locked plate external fixation does offer several advantages.10,11 The most significant advantage is the ability to provide more stability and support by allowing for the placement of multiple screws in fractures involving joint surfaces. Additionally, locked plate external fixation is known for its convenience in daily life.
In the present case, locked plate external fixation was appliedduring bone callus formation stage to replace the traditional external fixation for the treatment of a complex open tibial plateau fracture. The approach not only successfully achieves fracture healing but also preserves knee joint function.
Case presentation
A 55-year-old male patient was admitted to the hospital due to a construction collapse, which resulted in pale face, cold limbs, and continuous bleeding from the right lower leg for 7 hours. The initial diagnosis at another hospital suggested amputation, but the patient and his family refused and transferred him to our hospital.
During the preoperative examination,the patient exhibited a pale face and cold extremities, accompanied by abnormal movement in his right lower leg. There were two large wounds that were continuously bleeding, with exposed bone. The affected area also displayed swelling, tenderness, and positive percussion pain (Figure 1A). The dorsalis pedis artery pulses were weak in the injured limb.X-ray examination conducted at the another hospital revealed a fracture of the right tibia and fibula, with severe comminution of the tibial plateau. The fracture extended to the middle and lower tibia (Figure 1B, 1C).
_photographs_of_the_body_after_injury._(b_c)_preoperative_anterolateral_radiograph_of_t.jpeg)
Ethical Considerations
We present a case report that doesn’t require ethical review or approval. We ensure that the patient has already been informed and consented to the protocol management and publication in Orthopedic Reviews Journal.
Management and Outcomes
The patient underwent four surgeries in total.
During the first surgery, the patient received blood transfusion to correct the state of shock and underwent repair of the right anterior tibial artery. Thorough wound debridement was performed, along with external fixation using transarticular joint external fixator. Additionally, vacuum-assisted closure was implemented(Figure 2A,2B).
_postoperative_anterolateral_radiograph_of_the_right_lower_leg_after_the_first_surger.tiff)
During the second surgery, the right fibula fracture was reduced and internally fixed with Kirschner wires. The right tibia fracture was partially reduced and internally fixed with Kirschner wires as well. The external fixator of the right lower limb was adjusted, and the wound was thoroughly debrided and closed(Figure 3A,3B).
_postoperative_anterolateral_radiograph_of_the_right_lower_leg_after_the_second_surge.tiff)
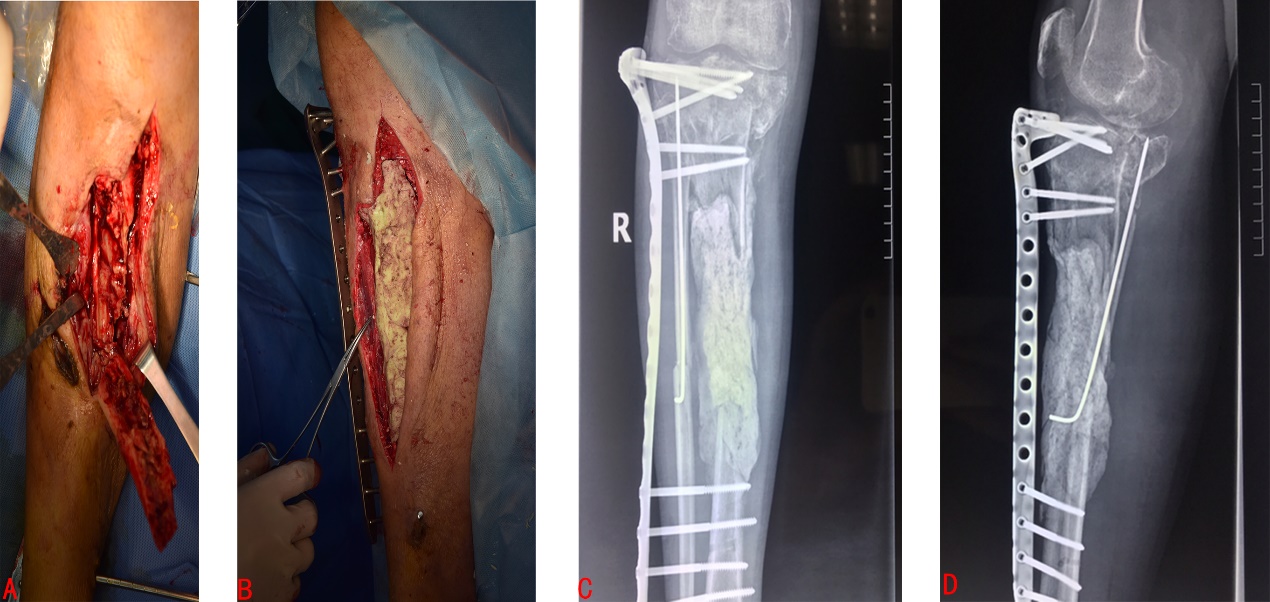
During the third surgery, which took place one month after the second surgery, a sinus tract with purulent discharge was observed in the anterior aspect of the right lower leg. The wound secretionculture results indicated an infection caused by Staphylococcus aureus. The patient underwent treatment with Masquelet technique for the tibial bone infection. The infected area was meticulously debrided and subsequently filled with antibiotic bone cement that had been mixed with vancomycin. Instead of using a transarticular joint external fixator, a tibial locked plate external fixation was utilized(Figure 4A, 4B, 4C, 4D).
_the_condition_of_the_bone_infection._(b)_the_bone_defect_area_was_filled_with_antibiot.jpeg)
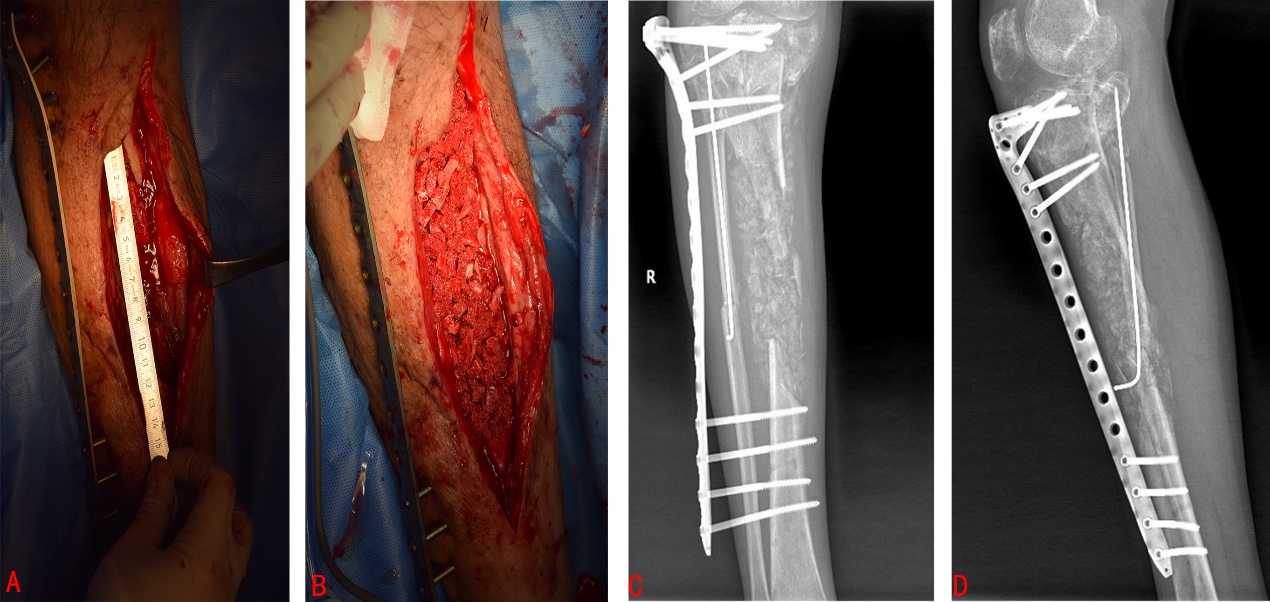
During the fourth surgery, which took place eight weeks after the first stage of Masquelet technique, a second stage of Masquelet technique was performed. The external locked plate fixation was not replaced. The patient underwent autogenous bone grafting from the bilateral posterior iliac crest and the right anterior iliac crest. The harvested autogenous bone was then mixed with four packets of allograft bone and implanted into the defect area (Figure 5A, 5B, 5C, 5D).
_masquelet_induction_membrane.(b)_the_defect_area_was_filled_with_both_autograft_and_al.jpeg)
At 1-year postoperative follow-up, the fracture ends have healed, and external fixation plate are stable in position (Figures 6A, 6B). At 5-year postoperative follow-up, the tibial defect has completely healed, but there is narrowing of the knee joint space (Figures 6C, 6D).The right knee joint has a clinical score of 95 points according to the Keen Society Score, and a functional score of 50 points (Figures 6E).
_postoperative_anterolateral_radiograph_of_the_right_leg_taken_one_year_after_the_bon.jpeg)
Discussion
The principles of trauma orthopedic injury control treatment state that the priorities are as follows12: saving lives, salvaging limbs, preserving limb function. The patient presented with hemorrhagic shock upon admission, therefore the primary focus was on saving their life. Emergency surgery was performed to address the fracture, and temporarytransarticular joint external fixation was applied to stabilize the fracture ends. Additionally, vascular and neural exploration was conducted to assess and address any potential damage to blood vessels and nerves in the area. The wound was then closed with vacuum-assisted closure.
Lower limb fracture reduction standardsrequire that the angular deformity be less than 10° and the displacement distance of the fracture ends be less than 0.5cm in adult.13 Additional, anatomic reduction is required for fractures involving the articular surface.14The initial postoperative X-ray of the patient showed that the angular deformity was greater than 10°, the displacement of the fracture ends exceeded 0.5cm, and the articular surface was irregular. Therefore, neither the lower limb fracture reduction standards nor the articular surface anatomic reduction standards were met.Considering the current issues with the patient, there are several factors to take into account. Firstly, the tibial plateau fracture is severely comminuted, making it difficult to achieve the desired outcome even with open reduction and internal fixation using plates. Secondly, tibial plateau fracture in the case is an open fracture, which significantly increases the risk of infection when internal fixation is performed. Lastly, if long-term transarticular joint external fixation is performed, the knee joint function will be compromised.
Regarding the above issues that exist after the first surgery, our team has decided to forgo anatomical reduction of the tibial plateau articular surface. In the event of post-traumatic arthritis, joint replacement surgery can be considered as a remedial option. To address the issue of long-term knee joint dysfunction caused by prolonged transarticular external fixation, our team has devised a solution. After 4 weeks of external fixation, during the bone callus formation stage when the tibial plateau bone fragments have formed a solid callus and are connected together, we will utilize the locking plate external fixation technique to replace the transarticular external fixation. This approach not only reduces the risk of infection but also preserves partial joint function. Additional, for fracture alignment and angular correction, a simple fixation with Kirschner wires can be used after reduction.
Based on previous research findings, the estimated incidence of postoperative infection in open tibial plateau fractures treated with internal fixation is approximately 8%.15The patient in this case developed a bone infection in the tibia one month after the injury, and the identified pathogen responsible for the infection was Staphylococcus aureus. Bone infection at this stage presents a tremendous challenge in terms of treatment for the patient. Given the severe fragmentation of the tibial plateau and the inability to satisfy the requirements for the Ilizarov technique at the proximal end,16 our team ultimately decided to utilize the Masquelet technique for the treatment of tibial bone infection. Regarding the choice of fixation devices, following the principles mentioned earlier, our team applied locked plate external fixation technique during bone callus formation stage to replace transarticular external fixation.
Conclusion
After the diligent efforts of our team, the patient ultimately achieved satisfactory results. The application of locked plate external fixation technique during bone callus formation stage to replace transarticular external fixation for the treatment of this complex tibial plateau fracture is the embodiment of precision medicine technology. The approach is worth considering and learning from for orthopedic clinicians when treating complex intra-articular fractures.
Author Contributions
All authors had full access to the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.Conceptualization, Wei Li and Quankui Zhuang; Methodology, Wei Li and Yong Chen; Investigation, Wei Li; Writing—Original Draft, Wei Li; Writing—Review & Editing, Quankui Zhuang; Visualization, Quankui Zhuang; Supervision,Quankui Zhuang.
Conflict of Interest Statement
All the authors declared that they had no conflict of interest in this case report.
Funds
This work was supported by program funded Fuyang Municipal Health Commission of China (No. FY2019-064 and No.FY2021-051).
Explanation of Data Replication
The data for this paper can be queried in the Chinese Medical Case Repository. http://journal.yiigle.com/LinkIn.do?linkin_type=cma&DOI=10.3760/cma.j.cmcr.2023.e01878.