Introduction
Ankle arthrodesis is a cornerstone limb-salvage procedure for patients with end-stage ankle arthritis, deformity, infection, or prior failed ankle surgery. Its role is especially critical in medically complex patients, such as those with diabetes mellitus. In this setting, arthrodesis provides substantial pain relief, improves mechanical stability, and helps prevent the progression to major amputation.1,2 Although advances in fixation techniques and perioperative care have improved outcomes, diabetic patients persistently experience higher postoperative complication rates compared with non-diabetic counterparts.3,4 Despite this increased perioperative risk, limb salvage following ankle arthrodesis in diabetic patients remains high, with contemporary literature reporting salvage rates approaching 90% to 95%.5 Diabetes alone has been consistently identified as an independent risk factor for a multitude of postoperative complications following ankle arthrodesis.6 Reported complication rates are approximately two- to four-fold higher in diabetic patients compared with non-diabetic patients.6,7
Outcomes in patients with diabetes vary, with comorbidities affecting postoperative risks.8 Diabetic peripheral neuropathy is a common long-term complication of diabetes that becomes more prevalent with longer disease duration and poorer glycemic control7,9,10 and may progress to Charcot neuroarthropathy.1,5,11 It strongly predicts adverse outcomes after foot and ankle arthrodesis, leading to higher complication rates, infections, and non-infectious issues than in diabetics without it.12 Neuropathy, characterized by a loss of sensation, altered biomechanics, and microvascular dysfunction. This leads to delayed healing and increased wound- and hardware-related complications, raising risks for construct failure, repeat surgery, and increased healthcare use post-arthrodesis.13 The risks are higher in patients with Charcot neuroarthropathy, who face more amputations, infections, wound issues, hardware removal, and kidney injuries than non-Charcot diabetics.9,11 Despite complications, ankle arthrodesis offers clinical benefits in diabetics, with fusion rates of 84%-96% and limb salvage rates of approximately 90% with proper fixation and technique.14,15 Functional outcomes improve post-arthrodesis in both diabetics and non-diabetics.14 However, diabetes leads to increased healthcare use, longer hospital stays, and higher non-home discharge rates.16 While studies have compared diabetic and non-diabetic outcomes post-arthrodesis, fewer have examined the impact of peripheral neuropathy in patients with diabetes.12 The link between diabetic neuropathy and infection, failure, reoperation, and mortality after arthrodesis has not been fully defined.
The purpose of this study is to compare postoperative complications, clinical outcomes, and healthcare utilization following ankle arthrodesis in diabetic patients with peripheral neuropathy versus diabetic patients without neuropathy. We evaluated postoperative infection, mechanical failure, revision arthrodesis, subsequent ankle surgery, emergency department use, and mortality over short- and long-term follow-up. We hypothesized that diabetic peripheral neuropathy would be associated with a greater short- and long-term postoperative burden following ankle arthrodesis, including higher rates of infection, failure-related complications, reoperation, mortality, and emergency department utilization.
Methods
Study Design and Data Source
This retrospective cohort study utilized a large healthcare database with deidentified patient-level data on diagnoses, procedures, prescriptions, and follow-up across multiple healthcare systems in the United States. Data were obtained from the TriNetX Research Network (TriNetX LLC, Cambridge, MA), a federated research platform aggregating EHR data from over 100 U.S. organizations. The analysis conducted included patients from January 2020 to January 2025. The study evaluated the association between diabetic peripheral neuropathy and postoperative outcomes following primary ankle arthrodesis. Outcomes were compared using CPT, ICD-10-CM, SNOMED, ATC, VA drug class codes, and TriNetX encounter definitions. As this study relied solely on aggregated, de-identified patient records without individually identifiable information, it was approved for exemption from Institutional Review Board approval by our academic institution.
Study Population
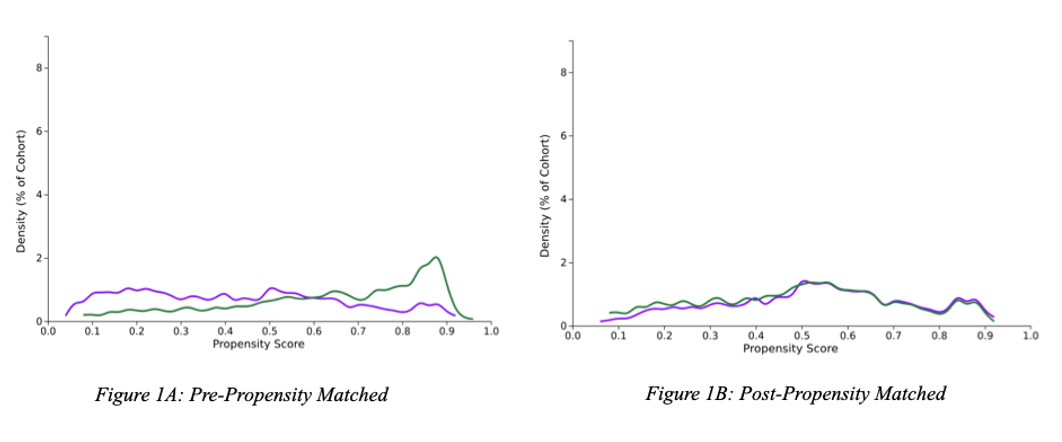
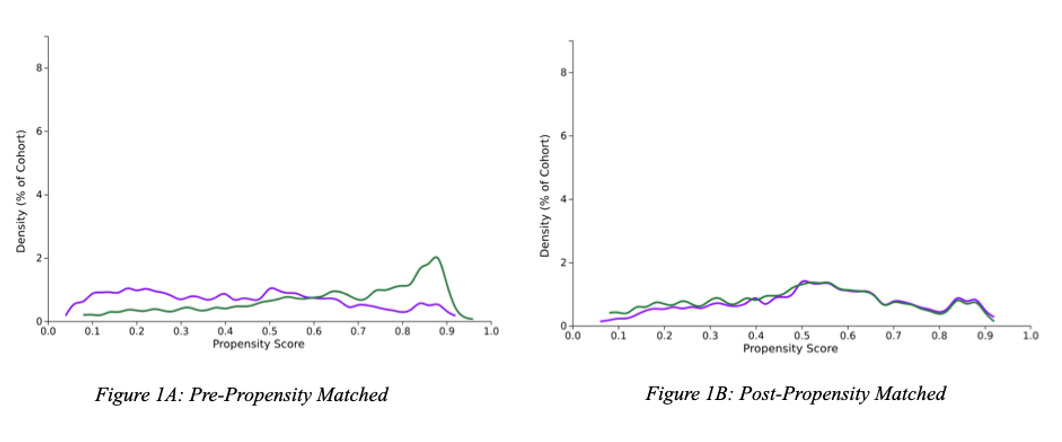
Adult patients undergoing ankle arthrodesis were defined using the procedural terminology record at the time of the index operation. To improve diagnostic specificity for the underlying operative indication, patients were required to have a diagnosis of primary osteoarthritis of the ankle and foot. Patients with diabetes mellitus were then stratified into two cohorts defined by neuropathy status. The diabetic neuropathy cohort included patients with diabetes and documented preoperative diabetic peripheral neuropathy. The diabetic non-neuropathy cohort included patients with diabetes but without documented neuropathy, excluding those with any diagnosis of diabetic neuropathy. Patients undergoing revision ankle arthrodesis or with indications related to trauma or malignancy were excluded. Only diagnoses recorded on or before the index ankle arthrodesis were considered for cohort assignment. Propensity score matching was performed 1:1, yielding 731 patients in each cohort. Full cohort-definition codes and exclusion criteria are provided in Supplementary Table 1.
Outcomes
The primary outcomes of interest were mechanical failure, revision arthrodesis, and any subsequent ankle surgery, as these represent principal structural and failure-related endpoints following ankle arthrodesis. Secondary outcomes included the remaining postoperative events assessed in this study, including venous thromboembolism (VTE), postoperative infection, myocardial infarction, mortality, and emergency department utilization.
All outcomes were assessed as postoperative events occurring after the index ankle arthrodesis and were defined using coded diagnoses, procedures, encounters, and mortality records available within the database. Mechanical failure was defined as a composite outcome using diagnosis and procedure codes associated with pseudarthrosis after fusion, implant-related complications, fracture-related complications, aseptic necrosis, and selected salvage or reconstructive lower extremity procedures. Revision arthrodesis was defined as any repeat ankle fusion procedure occurring after the primary indexed arthrodesis. Any subsequent ankle surgery was defined as any operative reintervention involving the ankle following the index arthrodesis, including incision, excision, arthroscopy, reconstruction, or revision procedures, repeat arthrodesis, and amputation-related interventions.
Medical complications included VTE, encompassing pulmonary embolism and deep venous thrombosis, postoperative infection, myocardial infarction, and mortality. Emergency department utilization was evaluated separately to capture postoperative healthcare use beyond surgical and medical complications. Full outcome definitions and associated code sets are provided in Supplementary Table 2.
Time-to-Event Assessment
Outcomes were assessed at 1, 3, and 5 years following the index ankle arthrodesis. This included VTE, postoperative infection, mechanical failure, revision arthrodesis, any subsequent ankle surgery, myocardial infarction, mortality, and emergency department utilization. Time-to-event was calculated from the date of the index ankle arthrodesis to the first occurrence of the outcome of interest, and patients who did not experience the event were censored at the time of death, last recorded healthcare encounter, or the end of the observation period, whichever occurred first.
Statistical Analysis
Baseline demographic and clinical characteristics were compared between the diabetic neuropathy and diabetic non-neuropathy cohorts (Supplementary Table 4). Postoperative outcomes were then compared between cohorts at each follow-up interval. Categorical outcomes were reported as event rates and compared using risk ratios with corresponding 95% confidence intervals. Mechanical failure, revision arthrodesis, and any subsequent ankle surgery were prespecified as primary outcomes, with statistical significance defined as a two-sided p-value <0.05. Remaining postoperative events were considered secondary outcomes and were evaluated using the Benjamini-Hochberg procedure to control the false discovery rate at a prespecified q-value of 0.05.
Results
1-Year Postoperative Outcomes
At 1-year following ankle arthrodesis, diabetic patients with peripheral neuropathy demonstrated significantly higher rates of several postoperative complications compared with diabetic patients without neuropathy. Postoperative infection was significantly more common in the neuropathy cohort (13.7% vs 7.9%; RR 1.724 [95% CI 1.269-2.343]; p<0.001). Mechanical failure was also significantly increased among patients with neuropathy (32.4% vs 23.5%; RR 1.378 [95% CI 1.165-1.629]; p<0.001). In addition, emergency department utilization was higher in the neuropathy cohort (26.0% vs 20.5%; RR 1.267 [95% CI 1.050-1.529]; p=0.013). After false discovery rate correction of secondary outcomes, postoperative infection and emergency department utilization remained significant. No significant differences were observed for VTE (4.8% vs 4.7%; RR 1.029 [95% CI 0.649-1.632]; p=0.902), revision arthrodesis (5.7% vs 4.2%; RR 1.355 [95% CI 0.862-2.130]; p=0.187), any subsequent ankle surgery (10.9% vs 9.0%; RR 1.212 [95% CI 0.890-1.652]; p=0.222), myocardial infarction (3.8% vs 3.0%; RR 1.273 [95% CI 0.735-2.204]; p=0.388), or mortality (4.2% vs 3.6%; RR 1.192 [95% CI 0.715-1.988]; p=0.499).
3-Year Postoperative Outcomes
At the 3-year follow-up after ankle arthrodesis, several complications remained significantly elevated in the diabetic neuropathy cohort (Table 2). Postoperative infection continued to be significantly higher in patients with neuropathy (16.1% vs 9.4%; RR 1.710 [95% CI 1.294-2.260]; p<0.001), as did mechanical failure (38.7% vs 29.1%; RR 1.329 [95% CI 1.149-1.536]; p<0.001). Emergency department utilization also remained significantly increased (34.6% vs 29.0%; RR 1.193 [95% CI 1.026-1.388]; p=0.021). Any subsequent ankle surgery was higher in the neuropathy cohort (15.2% vs 11.6%; RR 1.306 [95% CI 1.004-1.699]; p=0.046), although this difference did not remain significant after false discovery rate correction. Mortality was also higher (8.9% vs 6.2%; RR 1.444 [95% CI 1.002-2.830]; p=0.047), but this difference likewise did not remain significant after false discovery rate correction. In contrast, no significant between-group differences were identified for VTE (8.0% vs 6.7%; RR 1.204 [95% CI 0.836-1.734]; p=0.317), revision arthrodesis (8.1% vs 5.6%; RR 1.439 [95% CI 0.979-2.115]; p=0.062), or myocardial infarction (6.3% vs 4.4%; RR 1.438 [95% CI 0.926-2.231]; p=0.103).
5-Year Postoperative Outcomes
At the 5-year following ankle arthrodesis, diabetic patients with peripheral neuropathy continued to demonstrate a greater long-term complication burden. Postoperative infection remained significantly higher in the neuropathy cohort (17.8% vs 10.0%; RR 1.781 [95% CI 1.363-2.327]; p<0.001), as did mechanical failure (40.5% vs 30.5%; RR 1.327 [95% CI 1.154-1.527]; p<0.001). Emergency department utilization also remained significantly increased (37.5% vs 31.6%; RR 1.186 [95% CI 1.029-1.367]; p=0.018). In addition, revision arthrodesis reached statistical significance (8.3% vs 5.7%; RR 1.452 [95% CI 1.001-2.122]; p=0.049), and any subsequent ankle surgery was significantly more common among patients with neuropathy (17.0% vs 12.0%; RR 1.409 [95% CI 1.094-1.815]; p=0.007). Mortality also remained significantly elevated in the neuropathy cohort (12.0% vs 7.5%; RR 1.600 [95% CI 1.161-2.205]; p=0.004). After false discovery rate correction of secondary outcomes, postoperative infection, emergency department utilization, and mortality remained significant. No significant differences were identified for venous thromboembolism (9.7% vs 7.5%; RR 1.291 [95% CI 0.922-1.808]; p=0.136) or myocardial infarction (7.8% vs 5.7%; RR 1.357 [95% CI 0.923-1.995]; p=0.118).
Discussion
Principal Findings
The principal finding of this study is that diabetic peripheral neuropathy was associated with a consistently greater postoperative complication burden following ankle arthrodesis compared with diabetic patients without neuropathy. Across all postoperative follow-up intervals, patients with neuropathy demonstrated significantly higher rates of postoperative infection, mechanical failure, and emergency department utilization. Over longer-term follow-up, this risk extended to broader reoperation and survival outcomes, with any subsequent ankle surgery becoming significantly more common at 5 years, and both revision arthrodesis and mortality also reaching statistical significance by 5 years. Taken together, these findings suggest that diabetic peripheral neuropathy is not simply associated with isolated early postoperative complications, but rather with a durable and progressively increasing burden of structural failure, reoperation, and long-term morbidity following ankle arthrodesis.
Mechanical Failure, Subsequent Ankle Surgery, and Revision Arthrodesis
Clinically, this study found a progressive burden of construct-related complications in the neuropathy cohort. The composite mechanical failure outcome increased at 1-, 3-, and 5-year postoperative periods. Subsequent ankle surgery and revision arthrodesis also became more frequent at 5 years. These results suggest that neuropathy affects long-term mechanical durability beyond early wound-related risks. Diabetic peripheral neuropathy may impair early healing and create ongoing structural vulnerability, increasing the need for later operative intervention. By 5 years, over 40% of the patients experienced mechanical failure, 17.0% had subsequent ankle surgery, and 8.3% required revision arthrodesis. These rates are notably high and should be interpreted carefully. In particular, the composite mechanical failure outcomes were defined using coded variables rather than radiologically confirmed construct failure or nonunion alone.
As such, it captures a broader spectrum of failure-related events, including pseudarthrosis, implant-related complications, fracture-related complications, aseptic necrosis, and selected salvage or reconstructive procedures. Therefore, this rate should not be interpreted as a pure nonunion or hardware failure rate, but rather as a broader measure of the burden of structural complications after ankle arthrodesis. These outcomes, although not exclusive, indicate a substantial long-term burden of failure and reoperation. This underscores neuropathy as a determinant of long-term construct survivorship, not just as a perioperative risk. The elevated burden may reflect the combined effects of impaired bone healing, altered biomechanics, delayed recognition of complications, and the baseline complexity of patients undergoing ankle arthrodesis.9–13
These findings also parallel and extend the existing literature. Shibuya et al. demonstrated that diabetic peripheral neuropathy had the strongest association with bone-healing complications among evaluated risk factors in diabetic foot and ankle surgery, even after controlling for hemoglobin A1c levels.12 Similarly, O’Connor et al. identified peripheral neuropathy as an independent risk factor for persistent nonunion following revision arthrodesis. Importantly, they showed that neuropathy remained an independent predictor of revision failure even in non-diabetic patients.17 Hardware-related complications have also been reported more frequently in neuropathic patients; Wang et al. found that patients with diabetes-related Charcot neuroarthropathy had a 1.63-fold increased odds of hardware removal compared with non-Charcot diabetic patients.11 Therefore, our findings parallel and extend prior work, reflecting the combined influence of impaired bone healing, altered biomechanics, and increased construct stress in patients with diabetic peripheral neuropathy undergoing ankle arthrodesis.12,17
Infection and Healthcare Utilization
Postoperative infection was the major finding. Patients with neuropathy had higher infection rates, from 13.7% at 1 year to 17.8% at 5 years. This aligns with studies showing that diabetic neuropathy increases the risk of infection.18 In foot and ankle surgery, neuropathy increases the risk of infection beyond diabetes alone.10,19 In ankle arthrodesis, infection can cause wound morbidity, compromise fusion, increase implant complications, and lead to reoperations.6,10 Notably, patients with neuropathy had higher emergency department use at 1, 3, and 5 years, indicating broader postoperative issues such as instability, pain, and functional decline.20 This suggests that neuropathy affects surgical outcomes and long-term healthcare use, highlighting the importance of this study in focusing on value, resource use, and risk in complex orthopaedic cases.
Mortality and Broader Long-Term Risk
Mortality was significantly higher in the neuropathy cohort at 3 and 5 years, suggesting diabetic peripheral neuropathy’s impact extends beyond local surgical outcomes. Mortality after ankle arthrodesis likely involves many systemic factors not fully captured in a database study, but the divergence is clinically important. This finding should be interpreted cautiously, as the observed mortality difference is unlikely to be attributable to the arthrodesis procedure alone and more likely reflects the broader comorbidity burden and medical frailty of diabetic patients with peripheral neuropathy. It highlights neuropathy as identifying a more medically fragile subgroup of diabetic patients with not only higher local complication rates but also worse long-term outcomes.6 Because this study did not include a broader population comparator, it cannot determine the extent to which the observed 5-year mortality rate exceeds expected background mortality for similarly aged diabetic patients.
Strengths and Limitations
This study had several strengths. It uses a large multicenter database, employs propensity score matching to reduce baseline differences, and evaluates the outcomes over 5 years. It specifically examines neuropathy in patients with diabetic ankle arthrodesis, allowing for detailed risk stratification. Including both structural and nonstructural outcomes strengthens the analysis, offering a more comprehensive view than studies focusing solely on infection or union. However, this study has several limitations. As a retrospective database study, it is subject to coding errors, residual confounding, and limited clinical granularity regarding surgical technique, fixation strategy, neuropathy severity, glycemic control, radiographic fusion status, and postoperative management.
Neuropathy was treated as a binary-coded exposure, and the severity or duration of neuropathy could not be assessed, limiting the ability to determine whether more advanced neuropathic disease conferred proportionally greater risk. In addition, although propensity score matching improved balance across most measured covariates, hemoglobin A1c remained significantly different between groups after matching, and residual differences in glycemic control may therefore have contributed to the observed excess risk. Although some outcomes, particularly mechanical failure, were defined using coded proxies rather than direct radiographic confirmation, consistent findings across infection, mechanical failure, subsequent ankle surgery, revision arthrodesis, emergency department utilization, and mortality support this interpretation. Finally, the study period spanned January 2020 to January 2025 and overlapped with the COVID-19 pandemic, during which elective orthopaedic surgical volumes, follow-up patterns, and healthcare utilization may have been disrupted, particularly with respect to emergency department utilization.
Clinical Implications
Overall, the study suggests diabetic peripheral neuropathy is a key factor in early and late failure after ankle arthrodesis. The persistence of mechanical failure, increasing rates of subsequent ankle surgeries, and later divergence in revision arthrodesis and mortality indicate neuropathy worsens the long-term postoperative course. These findings impact preoperative counseling, risk stratification, perioperative optimization, and postoperative surveillance in diabetic patients considered for ankle arthrodesis. Patients with neuropathy should be informed that their risk extends beyond early complications to include long-term risks of structural failure, infection, and later reintervention.21,22 Neuropathy status should be part of decision-making when considering ankle arthrodesis versus alternatives like bracing, accommodative footwear, or primary amputation.20 Perioperative management may need modification in neuropathic patients. Meticulous soft-tissue handling, staged procedures, extended antibiotic coverage, careful fixation strategies, and intensified surveillance may mitigate risk.10,23,24 Closer follow-up, lower thresholds for advanced imaging, prolonged protected weight-bearing, and aggressive glycemic control optimization should be emphasized, as poor control may compound neuropathy-associated risk.10,25
Conclusion
In this propensity-matched analysis of diabetic patients undergoing ankle arthrodesis, peripheral neuropathy was associated with a significantly greater long-term burden of postoperative complications. Compared with diabetic patients without neuropathy, those with neuropathy demonstrated consistently higher rates of postoperative infection, mechanical failure, and emergency department utilization, with broader reoperation and survival differences emerging over time. Any subsequent ankle surgery became significantly more common by 3 and 5 years, while revision arthrodesis and mortality reached significance at 5 years. These findings suggest that diabetic peripheral neuropathy is a major determinant of both early and late failure following ankle arthrodesis and should be incorporated into preoperative counseling, perioperative optimization, and postoperative surveillance strategies.